Entomology and
Applied Science Letters
Applied Science Letters
 2023
Volume 10
Issue 2
2023
Volume 10
Issue 2

Despite 30 years of progressive legislation, most Indian women still lack access to safe abortion procedures. Our article presents a critical assessment of abortion services as well as a timeline of abortion-related laws and policies in India since the 1960s. In 2002 and 2003, the Medical Termination of Pregnancy (MTP) Act of 1971 was revised to improve the safety of services. These reforms included decentralization of abortion services to the district level, punitive measures to deter the performance of unsafe abortions, reduction of the physical specifications of facilities for providing early abortions, and legalization of medical abortion. This review article aims to provide a comprehensive analysis of abortion-related legislation and practices from different national perspectives. It suggests that there is no legitimate legal justification for the numerous complex rules and regulations surrounding abortion. Abortion is only considered safe when it is made available upon a woman's desire, widely available, inexpensive, as well as accessible.
INTRODUCTION
Throughout, both industrialized and developing countries, women, couples, and communities use induced abortion as a reproductive health treatment regardless of whether it is safe or hazardous, legal or illegal in cases where women lack access to trustworthy family planning tools, reproductive health care plays a crucial part in induced abortion. Women's health depends on the safety and accessibility of abortion services, and one step in ensuring these factors is to establish a favorable legal climate. Since 1971, India has allowed abortion on several grounds, becoming the second most populated nation on earth [1, 2].
|
|
|
Figure 1. The Medical Termination of Pregnancy (Amendment) Bill 2020 was approved by the Rajya Sabha, which would strengthen the secrecy clause and make it simpler for poor women to access complete abortion care. |
Since the passage of the Medical Termination of Pregnancy (MTP) Act, of 1971, Abortion has been recognized as legal in India but only in certain circumstances [3] under the Medical Termination of Pregnancy Act (MTP). Regulations (2003) were published to provide women with access to legal and safe abortion procedures. [4] The MTP Amendment Act 2021[5], which amended the MTP Act 1971, was passed in 2021 (Figure 1). These modifications included raising the gestational limit for some categories of women to 24 weeks, allowing women to access safe abortion services if their contraceptive has failed, and requiring up to 20 weeks of gestation for one abortion provider's opinion [6].
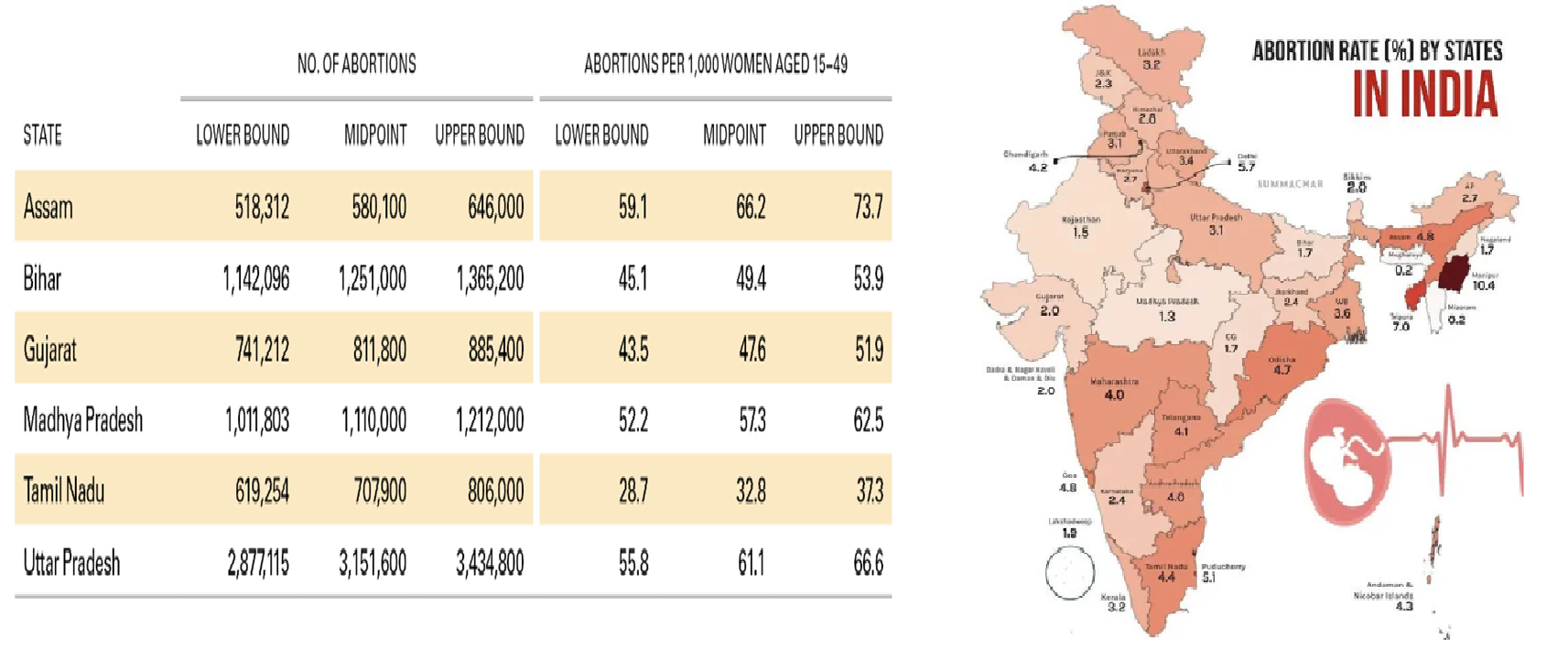
Results from the extensive study, Unintended Pregnancy and Abortion in India, at the state level, looked at six Indian states (UPAI). With a focus on Bihar, Assam, Madhya Pradesh, Tamil Nadu, Gujarat, and Uttar Pradesh. However, the research evaluates the frequency of abortions arising in the facility and non-facility locales. (Figure 2). It also offers reminiscent, extensive information on the entries of abortion-allied amenities (persuaded abortion and postabortion care) offered by the public as well as private division facilities, along with assessments of the levels of service-based refurbishment for women with complications associated with abortion [7].
Conclusively, it calculates the prevalence of unintended pregnancies using data on abortion rates.
|
|
|
Figure 2. Abortion rate (%) and Unintended pregnancies in six states of India. |
One of the concerns that has received a lot of attention at both the national and international levels is abortion. It has grown to be a contentious subject everywhere. Everyone is torn between believing that a mother has the freedom to end her pregnancy whenever she pleases and that an unborn child has a right to life.
The most fundamental of all human rights is the right to life, which has a fairly broad definition. According to Article 21 of the Indian Constitution, "No individual shall be deprived of his life and personal liberty except in accordance with the method established by law," the right to life has been acknowledged in India. Here, the term "person" refers to both genders. The right to an abortion is regarded as one of the most fundamental rights that women have among the other rights that they can exercise.
By identifying what is known and where there are knowledge gaps, this report provides an updated review of the state in the execution of engendered abortion in India. It does this by synthesizing recent studies on abortion. The following are some of the queries our review will address:
Despite more than 30 years of liberal laws, the majority of women in India still lack induction to safe abortion facilities. Nevertheless, the history of abortion law & policy bought reformation in India. Further, epidemiology and quality of care research performed since the 1960s, are all covered in this article. It analyses impediments to best practices and suggests making the necessary changes to policies and programs to increase access to secure abortion care.
RESULTS AND DISCUSSION
How did India's abortion law work during the 1960s?
According to Section 312 of the Indian Criminal Code, a woman who had an abortion before the 1960s may be sentenced to three years in prison and/or a fine (IPC). In the middle of the 1960s, the government formed the Dr. Shantilal Shah-led Shantilal Shah Committee and asked the group to look into the topic of abortions and assess whether India needed a law for the same.
In August 1971, the Parliament passed a medical termination law based on a proposal made to the Lok Sabha, Rajya Sabha, and the Shantilal Shah Committee. The 1971 Act on Medical Termination of Pregnancy (MTP) [8] initially applied to all of India, except for the state of Jammu and Kashmir, on April 1st, 1972.
Moreover, Section 312 of the Indian Criminal Code, 1860, classifies "causing miscarriage" as a crime, even when the pregnant woman consents to the miscarriage, barring circumstances in which the miscarriage is necessary to preserve the lady's life. This means that a woman may face charges for an abortion together with anyone else who aids it, such as a doctor.
Legal problems caused by moral dilemmas
The following situation may give rise to legal issues:
1994's pre-natal diagnostic technique act
Nonetheless, the Act on Pre-Natal Diagnostic Technique, which was passed in 1994 and later revised in 2003 and renamed as Act on Pre-Natal Diagnostic Technique (Prevention and Misuse) and Pre-Conception, was made possible through the mobilization of advocacy efforts by numerous civil society groups in the 1980s, even though India's sex ratio had been declining since the 1901 census. In-vitro fertilization institutions, genetic laboratories, and radiography are covered under the PCPNDT Act (including the use of ultrasonography).
The MTP and PCPNDT Acts address two entirely separate types of facilities without any cross-references, making their content quite distinct. But, when it comes to implementation, most authorities tend to mix the two when they refer to "preventing sex-selective abortions". These regulations were amongst many that were aimed at the welfare of women and girls, including laws barring child marriage, dowries, and equal inheritance rights. Yet, the lack of strict implementation and the absence of a plan to address ingrained cultural and societal beliefs have led to little improvement in the current situation.
As of 2020, there were 108.18 men for every 100 women in India's total population. There are 717,100,970 or 717.10 million men and 662,903,415 or 662.90 million women in India. Women make up 48.04 percent of the population, while men make up 51.96 percent. India has the biggest proportion of men overall, with 54.20 million men. India ranks 189th out of 201 countries and territories in terms of the gender ratio. It ranked 42nd among Asian nations out of 51 countries and territories.
For the 20–24 age group, the male-female ratio is at its greatest point, 112.54. India has the eighth-most skewed child-sex ratio, with 110.37 males for every 100 girls in the 0–14 age group. Men outnumber women 108.89 to 1 for those between the ages of 15 and 64 and 93.4 to 1 for those over 65. In India, there are more men than women under the age of 70. For centenarians, women outnumber males by a 2-to-1 ratio (Table 1).
The gender ratio in India is 943 females for every 1000 males, according to the 2011 Census. In urban areas, there are 929 females for every 1000 males, compared to 949 females for every 1000 males in rural areas. Males outnumber females in rural India by 21,813,264 and in urban India by 13,872,275 (Figure 3).
|
|
|
Figure 3. UN World Population Prospects 2019 on the sex ratio of the total population in India. |
Table 1. Depicts Estimated Indian sex ratio from 1950-2023.
|
India's Sex ratio estimates |
|||
|
Year |
Male |
Female |
M per 100 F |
|
1950 |
193,108,098 |
183,217,102 |
105.399 |
|
1951 |
196,321,041 |
186,055,904 |
105.517 |
|
1952 |
199,733,944 |
189,065,132 |
105.643 |
|
1953 |
203,320,096 |
192,224,269 |
105.772 |
|
1954 |
207,059,894 |
195,518,700 |
105.903 |
|
1955 |
210,940,825 |
198,939,781 |
106.033 |
|
1956 |
214,957,773 |
202,485,038 |
106.160 |
|
1957 |
219,112,756 |
206,157,953 |
106.284 |
|
1958 |
223,413,885 |
209,967,093 |
106.404 |
|
1959 |
227,873,797 |
213,924,774 |
106.521 |
|
1960 |
232,504,739 |
218,042,936 |
106.633 |
|
1961 |
237,313,422 |
222,328,744 |
106.740 |
|
1962 |
242,296,455 |
226,780,736 |
106.842 |
|
1963 |
247,438,408 |
231,387,194 |
106.937 |
|
1964 |
252,717,318 |
236,130,821 |
107.024 |
|
1965 |
258,120,909 |
241,002,419 |
107.103 |
|
1966 |
263,638,006 |
245,993,503 |
107.173 |
|
1967 |
269,283,162 |
251,117,415 |
107.234 |
|
1968 |
275,100,846 |
256,412,988 |
107.288 |
|
1969 |
281,151,623 |
261,932,710 |
107.337 |
|
1970 |
287,477,050 |
267,712,747 |
107.383 |
|
1971 |
294,098,355 |
273,769,666 |
107.425 |
|
1972 |
300,998,426 |
280,088,829 |
107.465 |
|
1973 |
308,133,555 |
286,636,581 |
107.500 |
|
1974 |
315,439,599 |
293,362,996 |
107.525 |
|
1975 |
322,871,275 |
300,231,625 |
107.541 |
|
1976 |
330,405,801 |
307,224,284 |
107.545 |
|
1977 |
338,059,105 |
314,349,661 |
107.542 |
|
1978 |
345,870,441 |
321,629,374 |
107.537 |
|
1979 |
353,898,047 |
329,097,301 |
107.536 |
|
1980 |
362,179,435 |
336,773,402 |
107.544 |
|
1981 |
370,724,075 |
344,660,922 |
107.562 |
|
1982 |
379,503,283 |
352,736,215 |
107.588 |
|
1983 |
388,469,530 |
360,959,428 |
107.621 |
|
1984 |
397,556,538 |
369,276,873 |
107.658 |
|
1985 |
406,713,092 |
377,646,920 |
107.697 |
|
1986 |
415,921,170 |
386,054,080 |
107.737 |
|
1987 |
425,183,245 |
394,498,850 |
107.778 |
|
1988 |
434,493,475 |
402,975,463 |
107.821 |
|
1989 |
443,851,777 |
411,482,898 |
107.866 |
|
1990 |
453,257,379 |
420,020,420 |
107.913 |
|
1991 |
462,697,149 |
428,576,053 |
107.962 |
|
1992 |
472,162,606 |
437,144,412 |
108.011 |
|
1993 |
481,663,763 |
445,740,103 |
108.059 |
|
1994 |
491,216,887 |
454,384,941 |
108.106 |
|
1995 |
500,830,598 |
463,091,988 |
108.149 |
|
1996 |
510,502,547 |
471,862,701 |
108.189 |
|
1997 |
520,217,326 |
480,682,702 |
108.225 |
|
1998 |
529,954,039 |
489,529,547 |
108.258 |
|
1999 |
539,685,380 |
498,372,774 |
108.289 |
|
2000 |
549,387,864 |
507,187,684 |
108.320 |
|
2001 |
559,042,845 |
515,957,249 |
108.351 |
|
2002 |
568,640,650 |
524,676,537 |
108.379 |
|
2003 |
578,176,499 |
533,346,647 |
108.405 |
|
2004 |
587,649,484 |
541,973,982 |
108.428 |
|
2005 |
597,052,213 |
550,557,711 |
108.445 |
|
2006 |
606,386,475 |
559,099,816 |
108.458 |
|
2007 |
615,629,520 |
567,579,951 |
108.466 |
|
2008 |
624,720,983 |
575,948,779 |
108.468 |
|
2009 |
633,583,576 |
584,142,641 |
108.464 |
|
2010 |
642,164,181 |
592,116,982 |
108.452 |
|
2011 |
650,436,593 |
599,851,346 |
108.433 |
|
2012 |
658,420,351 |
607,359,892 |
108.407 |
|
2013 |
666,165,661 |
614,676,458 |
108.377 |
|
2014 |
673,747,770 |
621,852,998 |
108.345 |
|
2015 |
681,223,332 |
628,929,060 |
108.315 |
|
2016 |
688,604,687 |
635,912,563 |
108.286 |
|
2017 |
695,880,522 |
642,796,257 |
108.258 |
|
2018 |
703,055,580 |
649,586,703 |
108.231 |
|
2019 |
710,129,572 |
656,288,184 |
108.204 |
|
2020 |
717,100,970 |
662,903,415 |
108.176 |
|
2021 |
723,973,437 |
669,435,596 |
108.147 |
|
2022 |
730,746,615 |
675,885,166 |
108.117 |
|
2023 |
737,408,384 |
682,247,416 |
108.085 |
Role of reproductive autonomy in abortion
In the Puttaswamy decision (Judge K. S. Puttaswamy v. Union of India), the fundamental freedom of women to choose their reproductive options was particularly acknowledged as a component of personal liberty under Article 21 of the Indian Constitution. 2012a: Paragraph 72; 2012b: Paragraph 46; 2012c: Paragraph 38) [11]. The panel also reaffirmed the viewpoint taken by a three-judge panel in Suchita Srivastava v. Chandigarh Administration (2009), [12-14] which held that a woman's right to reproductive freedom includes the right to carry a pregnancy to term, give birth, and raise children afterward and that these rights are an integral part of her right to privacy, dignity, and bodily integrity.
The Medical Termination of Pregnancy Act, 1971 (MTP Act), which controls abortions in India, came up in the Suchita Srivastava case. The MTP Act, which was passed two years before the US Supreme Court's famous Roe v. Wade decision (1973), places restrictions on when and when abortions are permissible. Only licensed medical professionals are permitted to end a woman's pregnancy under Section 3 of the act if they have a good-faith belief that furthering the pregnancy would endanger the woman's life or gravely harm her physical or mental health, or that doing so would result in a child who would be severely disabled by physical or mental abnormalities.
Obstacles to providing abortion services
Like too much of India's health care, abortion treatment is still not given enough attention, particularly in the public area. Poor treatment and a lack of a strong work ethic in the public health sector, along with a lack of effective law (or the inability to put it into practice), have contributed to an unrestrained proliferation of the private sector's services, many of which have an exploitative nature. Despite India's progressive abortion policy and regulation, it is frequently difficult for these measures to truly provide access to safe abortion care due to incorrect and unnecessary practices.
The law gives state governments the authority to control abortion providers. Although states have modified these laws and regulations, there are differences in how they are interpreted and applied. Some States have added layers of extraneous procedures, delayed the regulatory process administratively, and implemented pointless measures to ensure safety and prevent unsafe abortions.
There are situations when the obstacles to abortion access are not made by law or policy but rather by the providers themselves. Contrary to popular opinion, abortion doctors frequently demand such consent because it is a "common belief of the law, even though unless the patient is a juvenile, the law does not require a spouse's consent or the approval of a third party for termination [15, 16]. The need to protect themselves from social and legal issues brought on by complications or deaths during abortions are just but a few of the excuses typically used by providers for the requirement of spousal consent including the poor social position of women and their dependence on their husbands.
Last but not least, access is further restricted by so-called informal charges levied by public sector providers or exorbitant pricing in the private sector that play on women's vulnerability and misunderstanding of the law, especially when the unexpected pregnancy is not socially acceptable [17].
Regulation and policy of abortion in the future
Recent legislative and policy changes, while hardly revolutionary, yet represent a step forward in protecting a woman's right to have a safe abortion procedure. Indian policymakers, medical associations like the Federation of Obstetrics and Gynecology Societies of India (FOGSI) and the Indian Medical Association (IMA), nongovernmental organizations (NGOs) (especially Parivar Seva Sanstha, CEHAT, Health Watch, and the Family Planning Association of India), and health activists have only recently been concentrating on improving access to safe and legal abortion services in India [18-21]. Given that everyone's right to health in society is a fundamental one, governments are required to guarantee it fairly and equitably [22, 23].
The goals and tactics specified in the Action Plan of India's National Population Policy, 2000, are aligned with many of their recommendations.
In comparison to many other nations, such as the United States, where abortion prohibitions are strictly enforced both historically and currently, India's legal system is generally regarded as progressive.
Furthermore, public policymaking needs to be seriously rethought to accommodate all the stakeholders and put a priority on women and their reproductive rights rather than setting boundaries that doctors cannot cross while performing abortions.
Further research gap
Several research gaps are shown in this analysis of the abortion-related literature in India. Initially, specific data on the overall number of abortions performed are required for each state, as well as by rural/urban location within each state. The proportion of communal or commercial amenities at every point affords abortion facilities together with various professional workers in those amenities.
Additionally, there is little data on modes in the accessibility as well as the availability of facilities for abortion in unlicensed private locale amenities or to comprehend by what means such amenities would have bought changes in response to current legislation changes. Parallel to this, nothing is known about how much medical abortion, which is available through both legal and unauthorized routes, has impacted the general rate of abortion. Information on supply-side issues needs to be immediately considered for better comprehension of abortion facilities that are managed in India and further to direct forthcoming policy actions targeted at expanding the availability and accessibility of safe procedures.
It is crucial to address the underlying factors that lead to gender bias and son preference, and this should be done in tandem with initiatives to increase access to secure treatments and eliminate misunderstandings and false information regarding the legality of abortion. More control over their reproductive health decisions will enable better access to information and services for women, as well as a better understanding of their rights and entitlements, which will encourage healthier outcomes.
Insights into policy
In the year 2014 recommended amendment to the MTP Act, which corrects various issues with the existing rules on the provision of abortion services, should be thoroughly considered before being enacted and put into effect. This amendment seeks to:
It may be necessary to clarify or amend the Preconception & Prenatal Diagnostic Techniques Act, which forbids antenatal diagnostic tests misappropriation, the publicity of such technologies for the purposefulness of sex determination, further disclosing the sex of a fetus to expectant parents, to certify that women and healthcare professionals are conscious that the law generally does not confine abortion.
Perspectives
Last but not least, despite considerable advancements, much work needs to be done to augment women's admittance to secure abortion amenities in India. The numerous reproductive health suggestions quoted in the contextual portion of this article demonstrate that biases continue and disproportionately harm women in the northern, eastern, and central regions. Amongst, rural women those who are generally and frugally disadvantaged are those who are juvenile or single, and those who are unmarried. The majority of people in India still have confined access to sexual and reproductive health services, including safe abortion, and early marriage is still a common practise practice. Women and girls also continue to face gender discrimination, including but not limited to sex-selective practises practices. There is only one thing that can be done to move in this direction, and that is to educate experts and decision-makers on abortion law and dispel myths about it. There is a need to raise knowledge of both contraceptive and abortion services in the broader context of sexual and reproductive health, especially among adolescents. This can be accomplished by integrating strategies and treatments within family structures, gender roles, and value systems.
The moment has come to abandon quick fixes solutions and rhetoric aimed at "saving the girl child" and acknowledge the necessity of approaching the problem on numerous levels. The difference will be made through effective reforms, interventions, and implementation. While laws like the PCPNDT Act should be put into effect, so too should the MTP Act, laws against dowry, to prevent child marriage, to provide education and employment for girls and women, to ensure equal inheritance, paid maternity leave, and many others to ensure that all factors determining girls' and women's welfare are addressed in a comprehensive and integrative manner.
Children and teenagers must have the chance to maintain their health to learn in secure and wholesome settings. Healthy children obtain superior academic performance which, is related to improved health in adulthood [25]. Early life experiences, such as having access to education and healthcare, are thought to be critical for a person's subsequent development [26]. The majority of avoidable health behaviors, which are frequently started at a young age and continue into adulthood, are also linked to premature deaths and disabilities [27, 28]. In 1995, WHO created the Global School Health effort to include more institutions that may be categorized as "Health-Promoting Schools" in line with this goal. A school that "constantly strengthens its capacity as a healthy setting for living, learning, and working" [6, 7, 9, 29] is referred to as a health-promoting school by WHO.
CONCLUSION
The 1971 MTP Act of India, which is still not fully implemented, serves as proof that legislation alone has a limited impact on health, as this study has demonstrated. To lessen morbidity related to unsafe abortion, it is essential to support access to safe induced abortion services and raise public understanding of abortion law, safe procedures, and permitted providers. Thus, our article provided updated information regarding abortion laws in India and its policy services with further safety practices to be followed at the school level to strengthen the physical and mental health of each individual.
ACKNOWLEDGMENTS: K. R. Padma and K. R. Don, have drafted the paper. All the authors have checked and approved it and are thankful to the Department of Biotechnology Sri Padmavati Mahila Visvavidyalayam (Women’s) University, Tirupati-India &Department of Oral Pathology and Microbiology, Sree Balaji Dental College and Hospital, Bharath Institute of Higher Education and Research (BIHER) Bharath University, Chennai, Tamil Nadu, India.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None
Roe v Wade (1973): 410 US 113.