Entomology and
Applied Science Letters
Applied Science Letters
 2023
Volume 10
Issue 1
2023
Volume 10
Issue 1

Research on the vaginal microbiota (VMB) began more than 150 years ago. Women's health and reproduction are significantly influenced by the vaginal microbiome. The vaginal microbiota plays a critical role in preserving vaginal health and safeguarding the host against illness. Understanding the variables that influence the stability of bacterial communities in the vagina may aid in identifying the likelihood of developing diseases that are harmful to women's health. Numerous microorganisms can be found in vaginal secretions, and the host feeds them nutrients for expansion and development. The menstrual cycle and sex hormones, contraceptives, and the vaginal microbiome all influence the risk of infection and disease, unfavorable pregnancy outcomes, and the success of fertility treatments. The likelihood of getting diseases such as STIs, bacterial vaginosis, fungal infections, premature birth, etc. increases as a result of changes in the vaginal environment caused by impaired vaginal contact with the microbiomes. Bacterial vaginosis microbiota has been linked to endometritis after elective abortions, pelvic inflammatory illness, vaginal discharge, and poor pregnancy outcomes. There is mounting evidence that the composition of women's vaginal microbiota has a significant impact on their sexual and reproductive health, including the risk of miscarriage, premature birth, and HIV infection. The main emphasis of this review is on the full impact of the microbial ecosystem of the human vagina and how they affect women's health and reproductive outcomes at different stages of the women’s life cycle, which includes various vaginal infections such as bacterial vaginosis, trichomoniasis, cervical and endometrial cancer, etc.
INTRODUCTION
Human development and defenses as a whole are significantly influenced by microbiota. The macroscopic host and its commensal symbiotic bacteria are both multicellular beings that exist as meta-organisms [1]. Viruses, fungi, bacteria, protozoa, and other microbial species are present in these complex microbial communities [2, 3]. These symbionts are crucial in regulating the majority of host physiology due to their exceptional enzymatic capabilities and potential to express ten times as many different genes as their host's genome [4]. The human microbiota encompasses the communities of microorganisms that reside in the human body and the microbiome represents the genetic profile of all such microorganisms taken collectively [5-7]. The complex symbiotic, commensal, and pathogenic microbial association that lives in and colonizes the human body is essentially represented by a component of the cumulative genome of the human species [8]. The human microbiome, which is made up of about 10,000 different species of bacteria, lives inside the human body, similar to how the mouth and gut each have a variety of unique microbial populations. Additionally, trillions of tiny microorganisms, such as fungi, viruses, and bacteria, live in the female vagina [9]. This review's goal is to give a thorough explanation of the vaginal microbiome. The characteristics of bacterial vaginosis (BV) are reviewed about female health, and a strong correlation between BV and many illnesses is characterized by the need for thorough, accurate, and state-of-the-art treatment that lowers the negative effects on health (Figure 1).
|
|
|
Figure 1. Main determinants of the composition of the vaginal microbiome |
RESULTS AND DISCUSSION
Vaginal microbiota- introduction
In 1892, German obstetrician and gynecologist, Albert Doderlein discovered a long, thick, motile, rod-shaped, gram-positive, non-spore-producing microorganism in the vaginal fluid, which led to the discovery of vaginal microbiota [10]. When this bacterium was first identified, it was known as Doderlein's bacillus; however, because of its capacity to make lactic acid, it was later renamed Lactobacillus. Doderlein also found that the absence of Doderlein's bacillus in the vaginal fluid was linked to puerperal fever and that Doderlein's bacillus had an antagonistic effect on Staphylococcus growth [11, 12]. These key discoveries laid the groundwork that Lactobacillus is the most common bacterium in the vagina and is essential for women's health. It is now commonly acknowledged that the vaginal microbiome is more diverse and active than previously thought as a result of the advent and rapid development of high-throughput sequencing technologies [13]. A non-Lactobacillus dominant vaginal microbiome has also been linked to several diseases, including STIs, gynecologic cancer, infertility, and preterm birth, according to several observational studies [14].
Microbial communities of vaginal microbiota
The vaginal microbiome is a complex and dynamic micro-ecosystem that continuously changes throughout a woman's whole life and during her menstrual cycle. A stratified squamous non-keratinized epithelium and cervicovaginal secretion make up the vaginal mucosa [15]. Understanding the nature of the human body requires a study of the human microbiome, which will help researchers establish whether the microbial communities in humans are uniform across the board or vary from person to person. Variations in the core microbiota have been suggested to be associated with changes in human health and the likelihood of contracting illnesses [16]. Bacteria are one of the many varieties of microbes that exist and are responsible for a major portion of all life on Earth. According to the thorough study of the human vaginal microbial community, the Lactobacillus bacterial species predominate in the vaginal composition in the majority of females. This particular group of bacteria acts as protective agents in the reproductive system, preventing the colonization of hazardous germs by releasing hydrogen peroxide and some other compounds, such as bacteriocins. Although they contain a diverse range of both strictly and facultative anaerobic bacteria, a sizable portion of asymptomatic and healthy women lack enough Lactobacillus sp. in their vaginal microbiota. As a consequence, it can be said that the human vagina contains many core microbiomes rather than just a single core microbiome [17, 18]. Moreover, one of the essential aspects influencing vaginal composition is ethnicity. Asian and Caucasian women have been shown to have much greater lactobacilli levels than Black and Hispanic women [19, 20]. However, it is yet unknown whether this variation in Lactobacilli levels is a result of genetic determinants or associated with various hygiene practices, particularly vaginal douching [21].
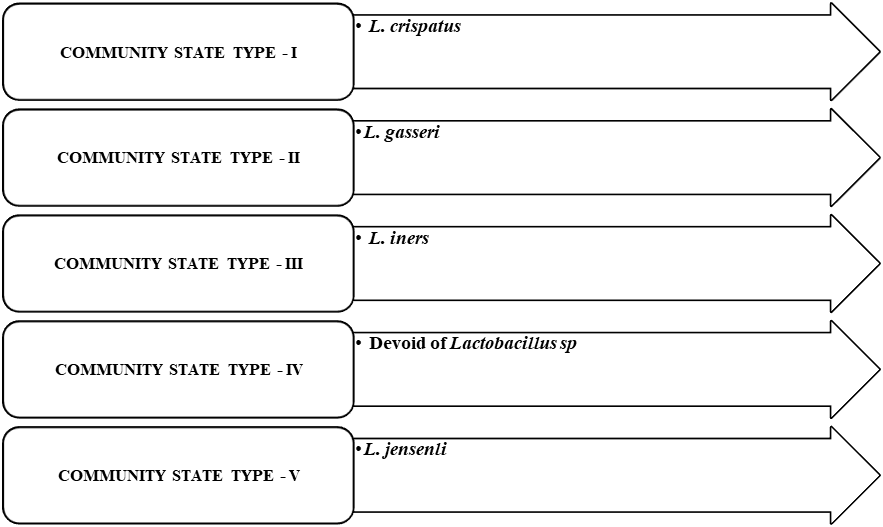
Researchers demonstrated that there exist five distinct classified microbial communities, or five different forms of Community State Types (CST), especially I, II, III, IV, and V as shown in Figure 2. Since no two females have the same vaginal environment, I assume it depends on which species of Lactobacillus plays a cent in these communities. Lactobacillus crispatus (L. crispatus) represents Community State Type I (CST I), Lactobacillus gasseri leads Community State Type II (CST II), Lactobacillus iners controls Community State Type III (CST III), and Lactobacillus jensenli dominates Community State Type V (CST V). Although Community State Type IV (CST IV) lacks Lactobacillus sp., it is incredibly rich in BV-associated strictly anaerobic bacteria such as Megasphera, Prevotella, Gardenella, and Sneathia [22].
|
|
|
Figure 2. Microbial communities of the vagina |
Throughout her lifetime, every woman appears to have the potential to transition from one CST state to another, with the transition from CST III to CST IV being the most common. Each species of Lactobacillus has distinct strengths and weaknesses [23, 24]. L. iners, for example, maybe more effective across a larger pH range, but they are unable to inhibit the growth of strict anaerobes, such as those found in CST IV. The concentration of lactobacilli drops with time, which shifts the balance of power so that the strict anaerobes take control even if L. iners cannot combat these anaerobes [25]. According to recent studies comparing the makeup of the vaginal microbiome from three vaginal sites, namely the cervix, mid-vagina, and introitus, the female vagina encompasses more than 200 phylotypes, with the most prevalent belonging to the phylum level Firmicutes, Bacteroidetes, Actinobacteria, and Fusobacteria (Figure 2) [26].
Composition of vaginal microbiota
The term "microbiota" refers to the complete population of microorganisms in a specific niche, such as the human stomach, mouth cavity, and vaginal area. The composition of the vaginal microbiota in a state associated with health and what transpires when changes in microbes, particularly significant changes in bacterial populations, occur (dysbiosis). The vaginal microbiota of healthy women appears to be dominated by Lactobacillus spp. The more common species are L. crispatus, L. gasseri, L. iners, and L. jensenii. Other species, however, are also found, though in smaller numbers. These include Fusobacterium, Bacteroides, Actinomycetes, Veillonela, Peptococcus, Propionibacterium, Staphylococcus aureus, Staphylococcus epidermidis, Peptostreptococcus, Viridans streptococci, Bifidobacterium, Enterococcus faecalis (Table 1).
Table 1. The principal micro-organisms present in the vagina throughout the female life cycle.
|
Women’s life cycle |
Microorganisms |
References |
|
Childhood |
Aerobic bacteria – S. aureus, S. epidermidis, V. streptococci, and E. faecalis Gram-positive anaerobic bacteria - Bifidobacterium, Peptostreptococcus, Peptococcus Actinomyces, and Propionibacterium Gram-negative anaerobic bacteria - Fusobacterium, Veillonella, Bacteroides |
Sgibnev et al. [27] |
|
Pre-puberty |
Gardnerella vaginalis, Prevotella bivia, and Lactobacillus are in relatively low numbers |
Shamasbi et al. [28] |
|
Puberty |
In Puberty: The most common species are L. jensenii, L. iners, L. crispatus, and L. gasseri |
Smith et al. [29] |
|
Adult |
L. crispatus, L. gasseri, L. iners, and L. jensenii are comparable to puberty |
Yamamoto et al. [30] |
|
Meno pause |
G. vaginalis, Prevotella, L. crispatus, and L. iners are the most common species. Candida, Mobiluncus, Staphylococcus, Bifidobacterium, and Gemella are less common |
Al-Baghdadi et al. [31] |
Factors influencing the vaginal microbiota
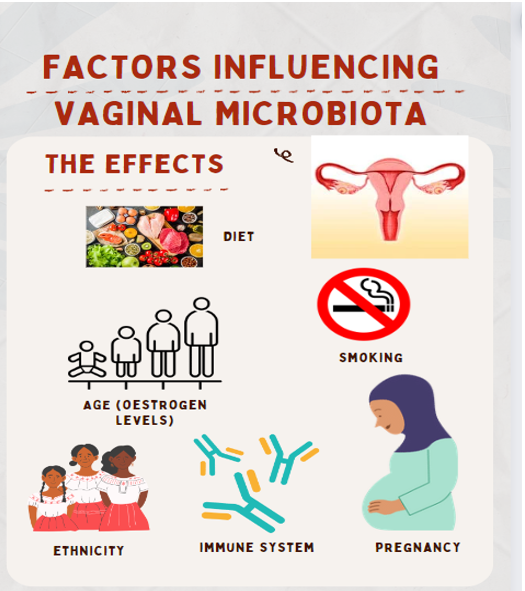
Even though the vaginal microbiota in healthy women has a comparatively small level of variety, it needs to be taken into account that its characteristics might alter throughout a woman's life and the menstrual cycle. As shown in Figure 3, age, ethnicity, and physiological elements including monthly hormone variations and the immune system all have an impact on the vaginal microbiota's extremely dynamic composition.
|
|
|
Figure 3. Factors influencing Vaginal microbiota |
Immune system
The vaginal mucosa's immune system simultaneously interacts with and regulates the Vaginal microbiomes (VMB) content [32]. Pro/anti-inflammatory cytokines/chemokines, secretory antibodies, epithelial and immunological cells, as well as antimicrobial peptides, all play a role in the complex interplay between the immune system and the VMB [33]. Epithelial and immune cells (dendritic cells) of the cervicovaginal mucosa simultaneously check for infections and maintain homeostasis with the VMB. These cells recognize microbial structures (antigens) through pattern recognition receptors such as Toll-like receptors (TLRs), which cause the production of antimicrobial peptides and immunomodulatory cytokines/chemokines. Dendritic cells also act as a crucial link between the innate and adaptive immune systems by dispersing antigens to immune cells such as macrophages, NK cells, neutrophils, T, and B cells [29].
Urbanization
Urbanization may also impact the VMB composition by increasing variety, however, the available data only includes a small number of ethnic groups [34]. There is evidence that among the socioeconomic determinants, education level may be related to VMB composition.
Age
Women change vaginal microbiota composition as they grow, and these changes are closely correlated with estrogen levels. Children's vaginal environments have a pH that is slightly alkaline (or neutral), and the majority of the microbiota is made up of gram-negative anaerobic bacteria like Fusobacteria, Bacteroides, and Veillonella as well as gram-positive anaerobic bacteria like Peptococcus, Actinomyces, and Pepto streptococcus [35]. In addition, low levels of estrogen and glycogen are seen in prepubertal girls, which are associated with thin mucosa, as well as low frequencies of P. bivia, G. vaginalis, and Mycoplasma hominis. During puberty, the vaginal epithelium builds up glycogen as a result of a process fueled by estrogen levels. Estrogen levels rise and glycogen deposits increase in the vaginal epithelium during puberty, which promotes the growth of lactic acid-producing bacteria. These bacteria create an unfavorable environment for pathogens by turning glycogen into glucose and then lactic acid, preventing infections and protecting the vaginal tract [36, 37]. Teenage girls' vaginal microbiome is similar to that of elderly women, with Lactobacillus spp. having a significant influence [38].
The plasma estrogen concentration is approximately 129 ng/L throughout the reproductive years, whereas the content is approximately 18 ng/L after menopause. On the other hand, estrogen levels in women decrease as they approach menopause [39]. As a result, the vaginal epithelium contains less glycogen, which in turn leads to a decrease in lactobacilli dominance. The pH of the vagina is raised because there are fewer lactobacilli than in prepubertal girls, which results in less lactic acid being produced. The alkalization of pH in the vaginal microbiota allows potential pathogens to enter or spread their colony there. Some accounts claim that the vagina is mostly occupied by Enterobacteriaceae and other fecal flora in an alkaline environment [40].
Ethnicity
In recent times, a variety of researchers have claimed that the ethnicity of the woman strongly influences the vaginal microbiota's composition, for instance, 396 North American women who appeared healthy and represented four ethnic groups had their vaginal microbiome evaluated by Ravel et al. [41] for variances (White, Black, Hispanic, and Asian). These researchers found that Asian and White women (80.2% and 89.7%, respectively) had higher vaginal bacterial populations of L. crispatus, L. gasseri, L. iners, and L. jensenii than did Hispanic or Black women. Asian and White women showed lower pH levels than Black and Hispanic women (5.0± 0.59 and 4.7 ±1.04, respectively), suggesting that this trend may be related to pH fluctuations. Asymptomatic Japanese women, White and Black women from North America, and the researchers' findings all showed considerably varied bacterial type frequencies. These authors claim that lactobacilli communities are present in 24.7% of Japanese women, 40.5% of Black women, and 13.3% of White women. Additionally, Black women lacked the broad lactobacilli communities that were found in White and Japanese women [42].
Diet
Diet influences the vaginal tract as well as the gut microbiota, as is well documented. More precisely, studies show that a balanced diet high in nutrients, low in fat, and with a glycaemic index may lessen the incidence of BV. In addition, consuming more micronutrients, especially calcium, vitamin A, and folate, may reduce the incidence of bacterial vaginosis (BV). Additionally, higher vaginal Lactobacillus spp. abundance is linked to diets high in betaine [43]. Though the sample size was limited, a recent study by Song et al. [44] found that vegetarian women had a higher total vaginal bacterial community than non-vegetarian women. Obesity-related dysfunction/disturbances in the host metabolism, and hormonal, and immune system modulation, which may influence the vaginal environment, are potential underlying causes. Moreover, the dysbiotic gut microbiota composition that is linked to obesity can further influence the composition of the VMB by acting as an "extravaginal source" for vaginal bacteria. Larger research examining the impact of different diets and/or body mass index (BMI) on particular CSTs is limited, nevertheless.
Smoking
cigarette smoking has been linked to a vaginal microbiome that lacks the protective effects of Lactobacillus spp. Brotman et al. [45] assessed the vaginal microbiota of 20 women who smoked and 20 women who did not. According to these investigators, smokers' vaginal microbiome had lower concentrations of Lactobacillus spp. than non-smokers did. Additionally, several studies have shown that smoking may increase the incidence of bacterial vaginosis in women. This increased susceptibility is probably due to smoking's anti-estrogenic effects and the presence of benzo[a]pyrene diol epoxide (BPDE), which has been found to encourage bacteriophage start in Lactobacillus spp. [46].
Pregnancy
In addition to changes in the endocrine, metabolic, and immune systems, pregnancy results in considerable alterations in the microbiota, including a decrease in overall diversity and enrichment with Lactobacillus species. Freitas et al. carried out a comparison study between pregnant and non-pregnant women [47]. These researchers found that compared to non-pregnant women, healthy pregnant women had a higher bacterial load and a lower concentration of Mycoplasma and Ureaplasma in their vaginal microbiota. Additionally, the investigators discovered that pregnant women had a higher prevalence of Lactobacillus species than did non-pregnant women. Pacha-Herrera et al. [48] found a similar result when they used sequence-based methods to determine Lactobacillus spp. constituted the majority of the vaginal microbiota in pregnant women. Surprisingly, during pregnancy, the pH dropped, the amount of vaginal discharge increased, and the vaginal microbiota also changed. An increase in Lactobacillus species could act as a defense against pathogens during pregnancy since, as already mentioned, they have antibacterial properties [49].
Vaginal douching
Vaginal douching is the practice of cleaning or cleansing the intravaginal area, ideally with a liquid solution. The purposes of douche use include keeping oneself clean, preventing infections by washing the vagina with douche products, particularly after having sex or menstruating, treating various illnesses, preventing pregnancy, and other cosmetic reasons. Douching exposes females to infections by eliminating the healthy vaginal microbiome and permitting the growth of harmful germs. Most research indicates that frequent vaginal douching raises the risk of pelvic inflammatory diseases, ectopic pregnancy, preterm birth, decreased fecundity, Chlamydia trachomatis illnesses, Herpes simplex type 2 disorders, and Bacterial vaginosis [50, 51].
Vaginal microbiota in different stages of life
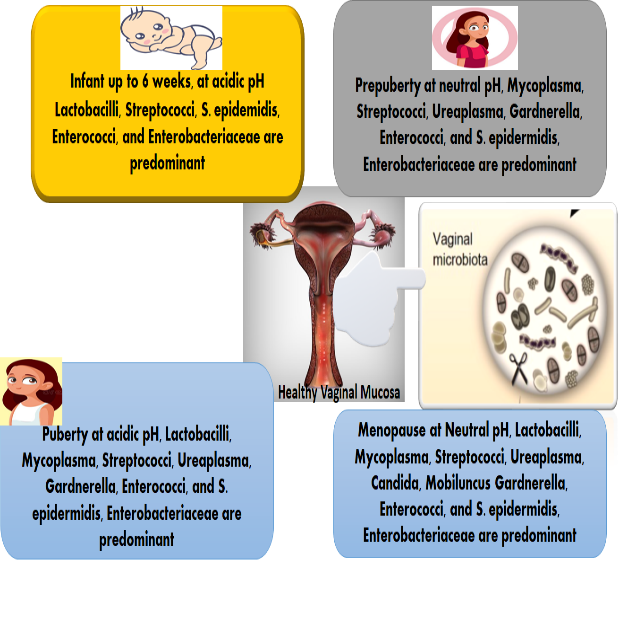
Along with changes in a female's physiology and reproductive status, the vital functions and microorganisms in the reproductive tract also change. The composition of the microflora in the entire reproductive tract is crucial for both the ability to conceive and the maintenance of pregnancy, according to the accumulating facts. According to research on IVF (In-vitro Fertilization), the type of microorganisms present in the uterus interact at the time of embryo transfer, resulting in the formation of pregnancy. As a result of persistent behavioral and hormonal abnormalities, the vaginal microbiome significantly improves during a woman's life (Figure 4) [52].
|
|
|
Figure 4. Composition of vaginal microbiota at different stages of the life cycle |
In healthy women
In contrast to the vast majority of human body sites where elevated concentrations of bacterial diversity are typically hypothesized to be a characteristic of health, female reproductive tracts are assumed to be somehow healthy and active even in low microbial diversity situations where only one or a few Lactobacillus sp. reign supreme. A typical, healthy vaginal microbiome is primarily composed of Lactobacillus sp., which acts as a protective barrier by thwarting several uropathogens. The commonly recognized theory of vaginal health states that these beneficial bacteria produce hydrogen peroxide, which helps to maintain the low pH environment required for defense against harmful pathogens. In addition to an acidic pH, the mucous membrane contact has other immunological mechanisms available to it under normal conditions [53].
Reproductive age of women
As a consequence of the enhanced estrogen levels, substantial quantities of glycogen, the preferred food supply for lactobacilli, are deposited in the vaginal walls. The lactobacilli-colonized vagina of new-borns who are still affected by their mothers' high estrogen levels has an acidic pH, but as time passes and the estrogen begins to leave their bloodstream, the lactobacilli population decreases and the vaginal pH environment becomes neutral [54, 55]. Women of reproductive age are more likely to suffer urogenital disorders as a result of an unbalanced vaginal microbiome [56]. When the chance of reproduction is greatest, just before menopause and after adolescence, there are many lactobacilli in the vaginal microbiome. Increased estrogen levels help to restore the advantageous vaginal lactobacilli and acidic pH environment that decrease during and after adolescence because estrogen levels have an impact on the entire vaginal microbiome. During the premenopausal period, estrogen promotes the colonization of the vagina by lactobacilli, which metabolize glycogen, produce lactic acid, and preserve intravaginal health by lowering intravaginal pH values [57].
Women during the menopause stage
Postmenopausal women frequently experience hormonal, sexual, and genital issues in addition to climacteric disorders like insomnia, hot flashes, and melancholy [58]. The vaginal microbiota has a significant impact on the state of a postmenopausal woman's life, including her sexual health, vaginal dryness, vulvovaginal atrophy (VVA), etc. When a woman reaches menopause, the decline in estrogen levels that results in vulvovaginal atrophy has a substantial impact on her vaginal flora. Vulvovaginal atrophy (VVA), which causes symptoms like sexual dysfunction, bleeding after physical intimacy, burning when peeing, discomfort, irritation, and irregular vaginal discharges with foul odors, is thought to affect 25–50% of postmenopausal females [59]. Estrogen activity has an impact on the major link between menopause and vaginal microbiota. The natural microbial populations convert glycogen, and estrogen promotes the maturation of the vaginal epithelium by causing a buildup of glycogen, which produces organic acids (mostly lactate) to protect the reproductive tract. In postmenopausal women, decreased estrogen production results in a decrease in lactobacilli and an increase in intravaginal pH, both of which promote the colonization of the vagina by pathogenic bacteria. Controversial estrogen helps postmenopausal women manage the symptoms of vulvovaginal atrophy (VVA), but in some cases, particularly in people with a history of active liver disease, breast cancer, prior venous thromboembolic stroke, or coronary artery disorder, hormone therapy (HT) has been seen to make up the vast majority. Vaginal lubricants can help with some vulvovaginal problems; however, they are damaging to the vaginal microbiome, lamina propria, and vaginal epithelium. Estrogen therapy has also been related to serious adverse effects such vaginal bleeding, chest pain, and episiotomy pain [60].
Influence on sexual health and reproductive health
The female vagina has a naturally low pH because of the presence of hydrogen peroxide and lactic acid generated by Lactobacillus sp. The vaginal microbiome is disrupted by the regular disturbances of the vaginal environment, including the use of various lubricants, sexual activity, semen, menstruation, antibiotics, and hormonal contraception [61]. In the case of gut bacteria, antibiotics are also responsible for eliminating lactobacillus, which allows dangerous pathogens to spread and grow [62]. Due to the reduction in Lactobacillus levels brought on by the use of conventional antibiotics, Pepto streptococcus anaerobic, G. vaginalis, Atopobium vaginae, Mobiluncus sp., Sneathia, Prevotella sp., Mycoplasma, Ureaplasma, and a variety of undeveloped or meticulous anaerobic organisms become much more energetic and can cause BV [63]. Therefore, a woman's reproductive health status can be inferred from the composition of her vaginal microbiome. Age also has an impact on the habitat of the vaginal microbiome [64]. As a result of the differences in microbial community composition among individuals, our understanding of the pathophysiology behind a wide range of illnesses, from atopic dermatitis to hepatocellular cancer, affecting certain areas of the body, is continually expanding [65, 66].
It has been demonstrated that the VM's structure affects IVF results, particularly diagnostic conception rate, implantation rates, and live birth rates, all of which are pertinent in uterine transplantation, where the live birth of a healthy infant is the main objective. Additionally linked to both premature and late miscarriage, and notably preterm birth is vaginal dysbiosis or lactobacillus depletion [47, 67, 68]. A healthful VM becomes much more lactobacillus dominant and much less diversified during pregnancy due to the impact of rising estrogen levels, but after delivery, when estrogen levels fall, many women acquire a lactobacillus-depleted or dysbiotic vaginal microbiome [35]. A lactobacillus-depleted or dysbiotic vaginal microbiome during pregnancy increases the risk of premature labor and, in particular, preterm prelabour barrier disruption. Contrarily, VM dominance of L. crispatus is generally prophylactic towards premature birth. A higher incidence of neonatal early-onset sepsis has been linked to Lactobacillus spp.-depleted or dysbiotic VMs [69, 70].
A healthy vaginal microbiota is essential for protecting against BV as well as other female reproductive illnesses like yeast infections, urinary tract infections (UTIs), sexually transmitted diseases (STDs), and more. Unbalanced vaginal microbiota frequently leads to vaginal infections, which can range from skin-related illnesses to potentially lethal disorders. For instance, a pregnancy-related streptococcus infection may result in circumstances that are lethal for the unborn child, and bacterial vaginosis may cause an early birth [71]. These infections necessitate prompt theragnostic, which entails a precise and expedient diagnosis followed by the appropriate course of therapy. If they are not promptly detected and treated, they might result in persistent vaginitis, pelvic inflammation, infertility, and endometriosis [72]. This section covers a variety of vaginal infections and ailments, including bacterial vaginosis, cytolytic vaginosis, vaginal candidiasis, and trichomoniasis.
Bacterial vaginosis disease (BV)
A disorder known as bacterial vaginosis (BV) affects the vaginal microbiome ecologically, upsetting the normal balance of the microbiota and causing an abundance of anaerobic bacteria. BV may manifest if some dangerous bacteria already present in the vagina—for example, G. vaginalis, Prevotella, and Morbiluncus bacterial strains, Atopobium vaginae, etc.—have a chance to thrive. It is associated with preterm birth, poorer pregnancy outcomes, the emergence of STIs and STDs (including Chlamydia trachomatis, HIV, Neisseria gonorrhoeae, and HSV-2), as well as other vaginal conditions. Due to the lack of a foreign pathogen (such as HIV or syphilis bacteria) linked with BV, it is not considered an STI or STD [73].
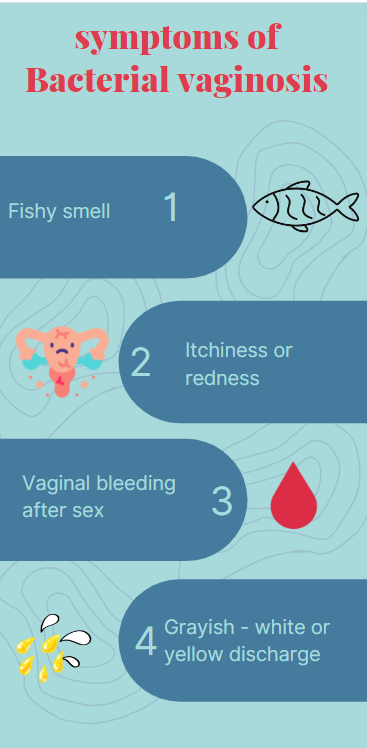
As seen in Figure 5, common symptoms of BV include itching, a foul odor, soreness, and a burning sensation. Thin, white discharge from the vagina is another sign [74]. Women of reproductive age are more prone to have BV because of unsafe sex, douching, having several sexual partners, and other poor lifestyle choices. Additionally, BV rates vary across individuals from different ethnic groups with different vaginal flora. As a result, it is possible to conceptualize BV as a multifactorial illness that is influenced by a complex interplay between microbial, individual, and environmental factors.
|
|
|
Figure 5. The figure depicts the symptoms of bacterial vaginosis |
Postmenopausal women are frequently reported to have BV due to huge colonies of anaerobic bacteria rather than lactobacilli in the vagina and higher vaginal pH (> 4.5) with more alkaline vaginal conditions. Both premenopausal and postmenopausal females have been reported to be affected negatively by this BV infection in terms of their gynecological and obstetric health. Although the recurrence rate is substantially greater and often occurs one year following therapy, antibiotics are typically used to treat it [75].
Cytolytic vaginosis
Other names for cytolytic vaginosis include Lactobacillus overgrowth syndrome and Doderlein's cytolysis. In typical circumstances, the female vagina has a significant amount of Lactobacillus, which aids in regulating the acidic pH microenvironment and releases lactic acid and hydrogen peroxide, an antibiotic. However, the overgrowth of these Lactobacilli results in a case of cytolytic vaginosis. Itching, vulval irritation (pruritus vulvae), burning or inflammation (vulvodynia and dysuria), and unpleasant sexual experience (dyspareunia) are all symptoms of lactobacilli overflow in the vagina. It is frequently misinterpreted as a fungal infection. Patients with diabetes mellitus (high blood sugar) are much more likely to contract this illness, and its symptoms are more pronounced when high levels of progesterone and estrogen occur in the luteal stage of the menstrual cycle [76].
Vulvovaginal candidiasis (VVC)
Candida sp. is the etiologic agent of vulvovaginal candidiasis (VVC), the second-most widespread and prevalent vaginal infection after BV. Premenopausal women with lower vaginal pH values (4.5) than BV are more susceptible to VVC than BV-positive women. Nearly 75% of fertile females get this illness just once throughout their lifetime. Uncomplicated VVC which is triggered by the Candida albicans (C. Albicans) species, typically affects non-pregnant women and results in mild to severe infections that can be cured with any antifungal medications [77]. Chronic and recurrent complex VVC is caused by non-C. albicans candidiasis. Complex VVC is more likely to develop in women of reproductive age, postmenopausal women who use exogenous estrogen, and women who have weakened immune systems [78]. Inflammation, edema, a cheese-like thick vaginal discharge, dysuria, and pruritus are typical signs of VVC [79]. Increased estrogen levels, diabetes mellitus, immunological state, and chronic antibiotic therapy are some of the potential causes for VVC formation, albeit the specific causes have not yet been determined (Table 2).
Table 2. Symptoms and causative agents of different vaginal infections
|
Infection |
Causative microbe |
Symptoms |
References |
|
Bacterial Vaginosis |
G. vaginalis, Prevotella, Atopobium vaginae, etc. |
Thin, pus-like white or yellow vaginal discharge with a foul fishy odor, vaginal irritation, and burning sensation during urination |
Van De Wijgert [80] |
|
Trichomoniasis |
Trichomonad |
Frothy yellow-grey-green vaginal discharge with a foul smell. Painful urination and sexual intercourse, vaginal soreness, redness, burning, and irritation |
McClelland et al. [81] |
|
Vulvovaginal candidiasis |
Yeast (Candida sp.) |
White, thick, crumbly, cottage-cheese-like vaginal discharge followed by vulval itchiness |
Disha and Haque [82] |
|
Gonorrhea |
Neisseria gonorrhoeae bacterium |
Creamy, watery, and slightly green vaginal discharge. Painful sexual intercourse, burning sensation during urination, frequent urination, lower abdominal pain, sore throat, and fever |
Konadu et al. [83] |
|
Cervical cancer |
Human papillomavirus (HPV) |
Pelvic pain, dark brown, reddish brown or red and watery vaginal discharge, painful intercourse with bleeding |
Champer et al. [84] |
Sexually transmitted diseases
Due to the diversity of microbial species found in the female reproductive tract, pelvic infections are very likely to occur. The vast majority of these pelvic infections are sexually contagious. Chlamydia trachomatis, Neisseria gonorrhoeae, Treponema pallidum, group B streptococci, Mycobacterium tuberculosis, human papillomavirus (HPV), human immunodeficiency virus (HIV), Cytomegalovirus, Herpes virus, and hepatitis B virus are a few potentially disastrous vaginal microscopic organisms that can cause deadly consequences [85]. Trichomoniasis, the vaginal microbiome, and the HIV connotation have been covered in this section.
Trichomoniasis
Trichomoniasis or Trichomonal Vaginitis is a form of STI that can affect females of any age, even teenagers. Trichomonad is the name of the parasite that causes this illness in a single cell. The vagina, urinary bladder, and urethra are all affected by this parasite, which can also affect the reproductive organ of both males and females. Patients who have this parasitic infection experience frothy yellow-grey-green vaginal discharge with an unpleasant odor. Other symptoms and indications include painful urination, uncomfortable sex, soreness, redness, burning, and irritation in the vagina. The use of latex condoms during sexual activity is the most efficient approach to avoiding this STI [86].
Risk of HIV and the vaginal microbiota
A woman's susceptibility to HIV may be made worse by imbalances in the vaginal microbiota and disruptions in the vaginal microbiome. Several studies have noted that a variety of vaginal microbial variations and the key bacteria concentrations are related to a higher risk of contracting HIV through several different potential pathways, including the yield of HIV-inducing factors, inflammation [87], or disrupting chemical and physical barriers to HIV [88]. Additionally, other vaginal infections including BV, which is marked by the presence of complicated anaerobic bacteria in the vagina, support HIV transmission [89]. Young South African women with very diversified vaginal microbial communities had an abundance of genital CD 4-positive T-cells that were activated, and as a result of a recent investigation, they had four times the risk of contracting HIV than women with less diverse and L. crispatus dominant vaginal microbiomes [90]. Additionally, the risk of contracting HIV is increased by the relative presence of several other bacterial taxa, including Sneathia sanguinegens, Mycoplasma, Prevotella melanogenic, P. bivia, and Veillonella montpellierensis [91]. By altering the vaginal microbiome, environmental, genetic, and behavioral variables are partly to blame for increased HIV risk. For example, using different vaginal products for hygiene reasons, using dry vaginal secretions to increase sexual enjoyment, and other such behaviors can all alter the pH of the vagina and have been linked to several infections that irritate and interrupt the vaginal-epithelial barrier and other symptoms.
Detection of the microbiota of the vagina
Bacterial communities are found inside the vaginal canal, according to numerous specialized investigations on the vagina and related microbiomes since the 1800s. At first, scientists employed traditional methods like light microscopy and gram staining to examine the microbiological makeup of the vagina. With the development of technology, culturing methods and PCR (Polymerase Chain Reaction) emerged, enabling researchers to more precisely and effectively discover and identify the numerous microbial species that inhabit the vagina. Even though the techniques for culturing produce reliable findings, they are slow and time-consuming, and only a small portion of the microbial species that have been properly identified yet have been cultivated in labs. Additionally, these techniques are not appropriate in the current environment to distinguish between the normal and pathological vaginal microbiome, necessitating the development of new methods for deeper taxonomic resolutions and functional investigation at the genomic level. However, false-positive and false-negative results challenge and restrict the use of PCR technology, which produces extremely sensitive information quickly. A dynamical and sophisticated system dominated by lactobacilli sp. has been shown to the globe by non-culture-based modern approaches [92]. Furthermore, the development of molecular-based tools has increased our understanding of the complexity and variety of vaginal bacterial microbiota. Sequencing methods have changed the study of the content and operational space of microorganisms in recent years. A culture-independent technology called 16S rRNA cloning and sequencing, which can identify a wide variety of vaginal microbiota and even discover uncultured taxa is constrained by low efficiency and expensive demand. Most diagnostic techniques for identifying various vaginal microbial communities include laboratory-based [93, 94] processes that are expensive, time-consuming, tedious, and call for professionally educated specialists. Therefore, it is essential to develop point-of-care (POC) microbial detection methods that are quick, portable, real-time, affordable, and sensitive. Due to recent advancements in nanotechnology and VLSI (very large-scale integration), the current research landscape has moved into the generation of biosensors and lab-on-chip technologies. The lab-on-chip POC platforms can be created for the full pathogenesis of many vaginal illnesses since it is possible to integrate various areas, such as microfluidics, biosensing, electronics, etc. on a single chip [87, 95, 96].
CONCLUSION
According to the aforementioned study, a woman's general health is significantly influenced by her vaginal microbiome. An understanding of the interaction between the female host and her vaginal microbiome can be gained by analyzing the fluctuations of vaginal bacterial diversity over the physiological phases of a female's life span. Therefore, to improve illness diagnoses, proper awareness of the vaginal microbiome composition in diverse settings and knowledge of numerous factors impacting such composition are essential. The present study in this field is on a thorough influence of the microbial ecosystem of the human vagina and how they affect women's health and reproductive outcomes in different stages of women’s life cycle which involves different vaginal infections such as bacterial vaginosis, trichomoniasis, cervical and endometrial cancer, etc. as well as the application of contemporary methods and the creation of compact and effective on-chip diagnostic equipment for the prompt identification of various vaginal infections and the evaluation of changes in vaginal microbiota.
ACKNOWLEDGMENTS: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None