Entomology and
Applied Science Letters
Applied Science Letters
 2023
Volume 10
Issue 4
2023
Volume 10
Issue 4

Malaria is the main public health issue in Ethiopia since it infects more than 75% of the country. This study's goal was to evaluate the risk factors for malaria in Dansha town and the area around it as well as the prevalence of the disease. Structured questionnaires and a Health facility-based study of confirmed malaria cases were conducted to determine the five-year (2012–2016) trend of malaria prevalence. To evaluate the data, SPSS version 20 was used. There were 28.4% more people who had malaria overall. The major plasmodium species identified was Plasmodium falciparum, followed by Plasmodium vivax. The prevalence of malaria parasite infections was significantly associated with age, while it was non-significantly associated with sex. Although the prevalence of Plasmodium falciparum was 3.413 times more likely to be higher than the prevalence of Plasmodium vivax among the age group under five years, the prevalence of Plasmodium falciparum was 0.793 times less likely to be higher than the prevalence of Plasmodium vivax among the age group from five to nine years. About 95% of the respondents had adequate knowledge about malaria. At the time of this study, 82.7% of the respondents had: a practice of using impregnated mosquito nets, 92.4% had risk factors for mosquito breeding sites near their homes, and 20.9% had headache symptoms. Health workers and responsible administrators should focus on giving health education about the prevention and control activities of malaria and how individual households use insecticide-treated nets correctly.
INTRODUCTION
Malaria is a parasitic disease caused by single-celled organisms called Plasmodium. It is transmitted to humans through the bite of infected mosquitoes. Malaria is a major cause of illness and death worldwide [1]. Malaria is a serious disease that affects millions of people around the world. In 2012, an estimated 3.4 billion people were at risk of malaria, and there were about 207 million cases and 627,000 deaths. Most of these deaths occurred in Africa. However, thanks to increased prevention and control measures, the mortality rate from malaria has decreased by 42% in the world and 49% in Africa [2].
Death and morbidity from Malaria have enormous social and economic costs [3, 4]. It causes poverty. Thus, it has a significant and measurable direct and indirect cost and has recently been shown to be a major constraint to economic development. Malaria may account for 40% of public health expenditure, 30%–50% of inpatient admissions, and up to 50% of outpatient visits in areas with high malaria transmission [5, 6]. It is estimated to cost Africa more than 12 billion United States dollars (USD) every year [7]. Additionally, malaria in Ethiopia has compelled people to live in the higher, less productive agricultural regions [8, 9]. Since agriculture is the foundation of the nation's economy and the peak season for malaria transmission occurs between planting and harvesting seasons, the disease has a significant negative influence on the economy [10].
Malaria is a major public health concern in Ethiopia, as it is in many other tropical countries [11, 12], 75% of Ethiopia's landmass is malarial, and 68% of its population is estimated to be at risk of malaria infection [13].
In Ethiopia, areas at altitudes between 1,600 and 2,000 m above sea level are epidemic-prone hypoendemic zones of malaria [14, 15]. Malaria prevalence has been found to vary among locations, possibly because of the country’s heterogeneous topography and weather conditions [16].
All population groups are affected by the erratic and seasonal transmission of malaria in Ethiopia. The key harvesting seasons of September to December and April to May coincide with the biannual malaria transmission peaks, which have substantial effects on the nation's subsistence economy. About 30% of all disability-adjusted life threats lost are due to malaria [17]. In 2009, malaria was the most common reason for people to seek medical attention in Ethiopia. It accounted for 12% of all outpatient visits and nearly 8.55% of all hospital admissions as per the Ethiopia Federal Ministry of Health (FMoH). The FMoH estimates that there are five to ten million clinical malaria cases and approximately 70,000 people die of malaria each year [10, 18]. It has also been documented in the nationwide child survival study that malaria affects school attendance by 20% and contributes to 47% of child deaths in Ethiopia [16]. However, given that a sizeable section of the population lacks access to healthcare services, these numbers may significantly underestimate the real burden of malaria in the nation.
Significant epidemics occur every five to eight years, with focal epidemics being the most common form. Large-scale malaria outbreaks struck 3368 places in 211 Districts in 2003 from April to December, resulting in two million clinical and confirmed cases and 3000 fatalities [16].
According to the Presidential Malaria Intervention (PMI), Plasmodium falciparum and Plasmodium vivax parasite prevalence in Ethiopia was 0.7% and 0.3%, respectively. According to the 2011 PMI draft report, 4.5% of children under the age of five tested positive for malaria using rapid diagnostic methods (RDTs), whereas 1.3% of children under the age of five tested positive using microscopy. Plasmodium falciparum constituted 77% of these infections. Thus, malaria is one of the serious public health problems that have a devastating impact on the socio-economic development of a country with a high mortality rate. People living in rural Ethiopia, especially in lowlands are most of the time infected by malarial disease with less knowledge and prevention methods.
Climate change is expected to have a direct impact on malaria by changing the behavior and distribution of mosquitoes, as well as the length of the parasite's life cycle. It is also expected to have an indirect impact by changing the ecological relationships between the organisms involved in malaria transmission (the vector, parasite, and host) [1]. At the Regional level, 75% of the area is potentially malarious [19].
Like in other parts of Ethiopia, malaria intervention and control activities have been scaled up. Malaria, however, continues to be one of the primary causes of morbidity in the area despite minor declines in prevalence [20].
According to the 2016/2009 health profile of the region, malaria is a leading cause of outpatient visits and admissions; approximately 58% of all suspected and confirmed cases of malaria occurred [21].
Malaria is one of the major public health issues in the research region as a result of these difficulties. To determine the prevalence of malaria and risk factors in Dansha town and its environs, this study was started.
MATERIALS AND METHODS
Description of the study area
The study was conducted at Dansha town and surrounding kebeles (lower administration units), Tsegedie District, Ethiopia. There are 25 kebeles in Tsegedie District. Tsegedie District has three climatic zones: Dega (highland) accounts for 33%, Weinadega (mid-land) constitutes 44% and Kola (low-land) accounts for the remaining 27% [22]. The area has two major rivers; Mekezo and Kaza. Dansha town and the surrounding kebeles such as Yekatit kebele, Alemgenet kebele, and Selam kebele have a total population of 27, 850 and 6328 households residing in an area of 3234 km2 making the population density of 16 people /km2. The town population accounts for 63.6% of the study area population. The temperature in the research region ranges from 30 – 40 °C. There is a District Hospital, a Health Center, four private clinics, three health posts, and six rural pharmacies in the research region. Dansha town has a total population of 17,712 and 4025 households and the surrounding administrative kebeles; namely, Yekatit kebele a population of 4555 and 1035 households, Alemgenet kebele a population of 4676 and 1063 households, and Selam kebele with a population of 907 and 205 households [23].
Study design, data collection instrument, and procedure
The study was carried out in Dansha town and surrounding kebele to estimate malaria prevalence and to identify risk factors associated with it. This was done through structured questionnaires and health institution-based treatment records from 2012-2016.
The data regarding the socio-demographic information and associated risk factors were gathered through means of a structured questionnaire and responses were obtained at the time of sample collection. Earlier to sample collection, precise explanations were given about the aim of the study for all households who are willing to participate in the study. Age, marital status, education level, knowledge, attitude, and practice regarding the participant's usage of bed nets were among the sociodemographic characteristics whose data were gathered. The general content of the questionnaire was well well-structured close-ended questionnaire. The questionnaire was prepared for each participant and filled by a representative of the sample selected households under the direct supervision of the data collector.
The questionnaire deals with an individual’s socio-demographic information, knowledge and use of preventive measures, use of anti-malarial drugs, and other malaria-related issues.
Sampling size and sampling techniques
To calculate the sample size, a confidence interval of 95% was used, along with the lowest acceptable result of 3% and a total of 384 houses. This number was then multiplied by 10% to account for non-response, yielding a total of 422 households. 16 of the 422 families that were expected to participate in the study were not included because they did not respond. A response rate of 96.2% was consequently attained. Four hundred and six volunteers participated in the study.
Thus, the sample size is determined by the following formula [24].
|
n=Z2P (1-p)/d2 |
(1) |
Where:
n = sample size for households
p = Average prevalence
d = Error value
z = Confidence interval z (95%) = 1.96
n = 384 members of households obtained
Contingency = 10% = 38 therefore, 384 + 38= 422
The study participants were selected using simple random sampling. Based on proportional sampling to population sizes in town and surrounding countryside kebeles, the study sample size was determined. In each household one randomly selected respondent was taken as a study subject. In this study, 270, 67, 70, and 15 respondents were selected from Dansha town, Yekatit, Alemgenet, and Selam kebele, respectively.
Inclusion and exclusion criteria and study variables
All household dwellers in Dansha town and its surrounding countryside were included in this study. Dwellers that are not present at the time of the study, those who were not volunteers, and dwellers of the town or surrounding countryside who did not live for at least one year were excluded.
The dependent variable of this study was the prevalence of malaria in the study. The independent variables were: socio-demographic characteristics, health information, type of living area, insecticide-treated bed net possession in households, and distance from mosquito breeding site.
Statistical analysis
Data was entered and analyzed by the SPSS version 20 software package. Descriptive statistics were used in the analysis for frequencies, and percentages, and binary logistic regression analyses were conducted to describe findings. P-value < 0.05 was considered statistically significant. The data were described and presented using tables and figures.
RESULTS AND DISCUSSION
Socio-demographic characteristics of respondents
In this study, 60.2% and 39.8% of respondents were males and females, respectively. The respondents' ages ranged from 18 to 67 years. Regarding marital status, about 31.8% of respondents were single, 60.7% were married, 5.2% were divorced and 2.4% were windowed. The distribution of the study participants based on their educational status showed that 43.4% of the respondents could not read and write, 7.6% of the respondents could read and write, 18.2% were in their elementary school levels, 19.9% were in their secondary school levels and 10.9% were holders of university diploma and above (Table 1).
Table 1. Socio-demographic characteristics of respondents in Dansha town and surroundings.
|
Characteristics |
Frequency |
Percentage |
|
|
Sex |
Male |
254 |
60.2 |
|
Female |
168 |
39.8 |
|
|
Age |
18-27 |
136 |
32.2 |
|
28-37 |
112 |
26.5 |
|
|
38-47 |
74 |
17.5 |
|
|
48-57 |
57 |
13.5 |
|
|
58-67 |
43 |
10.2 |
|
|
Marital status |
Single |
134 |
31.8 |
|
Married |
256 |
60.7 |
|
|
Divorced |
22 |
5.2 |
|
|
Widowed |
10 |
2.4 |
|
|
Religion |
Orthodox |
369 |
87.4 |
|
Muslim |
53 |
12.6 |
|
|
Educational status |
Unable to read and write |
183 |
43.4 |
|
Read and write |
32 |
7.6 |
|
|
Elementary |
77 |
18.2 |
|
|
High school |
84 |
19.9 |
|
|
College and above |
46 |
10.9 |
|
Knowledge of respondents on malarial disease
Knowledge of Respondents about malaria is shown in Table 2. About 95% of them heard about malarial diseases from different sources, such as Radio, Television, Health professionals, friends, and others. Many responders demonstrated an adequate understanding of malaria, including the accurate connection between the disease and mosquito bites, its possible effects, and the appropriate treatment choices. About 75.8% of respondents said they thought malaria could be spread from an infected person to a healthy person through mosquito bites; 6.9% said it couldn't; the remaining 5.2% said they didn't know; and the rest said it couldn't be spread from person to person. Regarding conditions that are associated with malaria infection, 84.1% of respondents knew that stagnant water and swampy areas were the main sites of mosquito breeding. Mosquitoes often bite at night, as almost 92.9% of respondents correctly identified. More than 75.4% of research participants thought malaria could be prevented, and almost all 85.3%- thought it could be cured. The most often reported malaria preventive strategies were the usage of bed nets and drying stagnant water. The government's enhanced efforts to promote health and the study's timing may be to blame for this. Regarding symptoms of malaria, the respondents said that about 10.9% fever, 19.4% shivering, 20.9% headache, 14.9% vomiting, 11.1% chill, 38.5% loss of appetite, 6.4% back pain, 6.6% joint ache, and 1.2% other as important symptoms of malaria in the research region.
Table 2. Knowledge of respondents about malaria at Dansha Town and its surroundings.
|
Knowledge |
Response |
Frequency |
Percentage |
|
Have information on malaria |
Yes |
401 |
95% |
|
No |
21 |
5% |
|
|
Is malaria a health problem in the study area |
Yes |
398 |
94.3% |
|
No |
24 |
5.7% |
|
|
Malaria is a transmittable disease |
Yes |
337 |
79.9% |
|
No |
44 |
10.4% |
|
|
I don’t know |
41 |
9.7% |
|
|
Malaria is transmittable by mosquito bite |
Yes |
320 |
75.8% |
|
No |
29 |
6.9% |
|
|
I don’t know |
22 |
5.2% |
|
|
When do mosquitoes bite mostly |
Night |
392 |
92.9% |
|
Day |
30 |
7.1% |
|
|
Know the breeding sites of mosquitoes |
Yes |
355 |
84.1% |
|
No |
67 |
15.9% |
|
|
Is malaria a curable disease? |
Yes |
360 |
85.3% |
|
No |
11 |
2.6% |
|
|
I don’t know |
51 |
12.1% |
|
|
Is there any method to prevent malaria? |
Yes |
318 |
75.4% |
|
No |
104 |
24.6% |
|
|
Symptoms of malaria - Fever - Chill - Headache - Shivering - Vomiting - Back pain - Joints ache - Loss appetite - Other |
|
46 47 88 82 63 27 28 36 5 |
10.9 11.1 20.9 19.4 14.9 6.4 6.6 8.5 1.2 |
Risk factors associated with malaria
Table 3 showed that about 14.2% of the respondents did not use mosquito nets, while 85.8% of the respondents used mosquito nets to protect themselves from the bite of mosquitoes. About 87.7% of the respondents do not use body oil like buzz off to prevent mosquito bites. Out of 422 respondents, 291 (69.0%) did not report malaria-associated problems to local health workers. In the study area, about 390 (92.4%) of respondents lived near mosquito breeding sites. Regarding housing conditions, 34.8% of them lived in houses that had thatched roofs, 57.3% lived in houses that had corrugated iron sheets, and 7.8% lived in houses that had concrete roofs. Regarding wall opening, 87.7% of them lived in houses with openings on the walls due to the high temperature of the area which may enhance mosquito entrance into the living room of households (Table 3).
Table 3. Risk Factors associated with malarial and the practice of the community to prevent malarial disease in Dansha town and its surroundings.
|
Risk Factor Variables |
Response |
Frequency |
Percent |
|
Use mosquito net |
Yes |
362 |
85.8 |
|
No |
60 |
14.2 |
|
|
Use body oil (buzz off) |
Yes |
52 |
12.3 |
|
No |
370 |
87.7 |
|
|
Report problems to local health workers |
Yes |
131 |
31.0 |
|
No |
291 |
69.0 |
|
|
Mosquito breeding site near the living room |
Yes |
390 |
92.4 |
|
No |
32 |
7.6 |
|
|
Type of roof of living room |
Thatched roof |
147 |
34.8 |
|
Corrugated iron sheet |
242 |
57.3 |
|
|
Concert roof |
33 |
7.8 |
|
|
Presence of a wall opening |
Yes |
370 |
87.7 |
|
No |
52 |
12.3 |
|
|
Prevention Variables |
|||
|
Community Campaign Activities to control the environment from mosquito |
Drain breeding sites |
317 |
75.1 |
|
Spray chemicals |
4 |
0.9 |
|
|
Clear vegetation |
13 |
3.1 |
|
|
Participate in health education |
88 |
20.9 |
|
|
Medical treatment |
Take prescribed anti-malaria drugs |
323 |
76.5 |
|
Use traditional medicine |
99 |
23.5 |
|
|
Method currently used |
Impregnated mosquito net |
349 |
82.7 |
|
Fumigation |
73 |
17.3 |
|
|
Reason for not using an Impregnated mosquito net |
Not available |
14 |
3.3 |
|
Not affordable |
9 |
2.1 |
|
|
Not aware of its use |
50 |
11.8 |
Practice of the community to prevent malaria
Some practices of respondents to prevent malaria are shown in Table 3. About, 75.1% drained breeding sites of mosquitoes. Among the respondents, 76.5% and 24.5% had a practice of taking prescribed anti-malaria drugs and traditional medicine, respectively. Three hundred forty-nine (82.7%) of respondents used impregnated mosquito nets while the remaining used fumigation. Out of those who used fumigation to prevent malaria, 3.3%, 2.21%, and 11.8% did not use mosquito nets and justified them as not available, not affordable, and did not know about their use, respectively.
Prevalence of malaria in Dansha town and its’ surroundings from 2012-2016
Trends of malaria infection among patients admitted at Dansha Town Health Center
From 2012 to 2016, 87.4% of Plasmodium falciparum and 12.6% of Plasmodium vivax were identified in clinical records from the Dansha District Health Center for Malaria. The overall prevalence of malaria in the whole health record was 28.4%. The prevalence of malaria was 28.7% in 2012, 25.7% in 2013, 25.9% in 2014, 28.5% in 2015, and 32.8% in 2016 (Table 4). The highest annual cumulative malaria prevalence, 32.8%, was detected in 2016. This was much greater than in 2012, 2013, 2014, and 2015. In the past five years of health records, malaria has been prevalent throughout the year; the peaks in prevalence were observed mostly from May to December. In 2016, high malaria prevalence was widespread throughout the year, while the lowest annual cumulative prevalence of 25.7% was detected in 2013. The prevalence of plasmodium falciparum cases increased from 2012 to 2014 by 56.2%, but in 2015, it decreased by 19.03%, and in 2016, it increased by 24.8% whereas the prevalence of plasmodium vivax increased from 2012-2015, but it was decreased in 2016 by 18.6%.
Table 4. Trends of malaria disease among patients admitted at Dansha Town Health Center were recorded from 2012 – 2016.
|
Year |
Parameters |
Jan |
Feb |
Mar |
Apr |
May |
Jun |
Jul |
Aug |
Sep |
Oct |
Nov |
Dec |
Total |
|
2012 |
No. examined |
645 |
572 |
502 |
732 |
713 |
664 |
510 |
626 |
625 |
701 |
722 |
907 |
7919 |
|
Positive |
202 |
131 |
112 |
223 |
205 |
157 |
134 |
151 |
212 |
250 |
239 |
260 |
2276 |
|
|
P. falcipirum |
155 |
110 |
89 |
167 |
143 |
127 |
98 |
119 |
215 |
202 |
205 |
195 |
1825 |
|
|
P.vivax |
47 |
21 |
23 |
56 |
62 |
30 |
36 |
32 |
17 |
48 |
34 |
45 |
451 |
|
|
2013 |
No. examined |
578 |
430 |
566 |
608 |
898 |
835 |
728 |
674 |
634 |
726 |
766 |
764 |
8207 |
|
Positive |
178 |
122 |
137 |
207 |
222 |
212 |
108 |
110 |
125 |
212 |
235 |
241 |
2109 |
|
|
P. falcipirum |
165 |
98 |
127 |
191 |
215 |
199 |
88 |
92 |
102 |
198 |
221 |
220 |
1916 |
|
|
P.vivax |
13 |
24 |
10 |
16 |
7 |
13 |
20 |
18 |
23 |
14 |
14 |
21 |
193 |
|
|
2014 |
No. examined |
725 |
676 |
754 |
822 |
864 |
777 |
568 |
478 |
467 |
688 |
674 |
656 |
8199 |
|
Positive |
247 |
204 |
216 |
226 |
238 |
204 |
116 |
89 |
84 |
128 |
174 |
202 |
2128 |
|
|
P. falcipirum |
222 |
192 |
201 |
212 |
218 |
185 |
95 |
74 |
71 |
114 |
154 |
190 |
1928 |
|
|
P. vivax |
25 |
12 |
15 |
14 |
20 |
19 |
21 |
15 |
13 |
14 |
20 |
12 |
200 |
|
|
2015 |
No. examined |
436 |
494 |
761 |
846 |
772 |
698 |
747 |
790 |
470 |
557 |
747 |
648 |
7966 |
|
Positive |
158 |
189 |
218 |
253 |
247 |
218 |
112 |
252 |
116 |
167 |
226 |
111 |
2267 |
|
|
P. falcipirum |
126 |
143 |
194 |
212 |
215 |
209 |
92 |
219 |
85 |
145 |
193 |
91 |
1920 |
|
|
P. vivax |
32 |
46 |
24 |
41 |
32 |
9 |
20 |
33 |
31 |
22 |
33 |
20 |
347 |
|
|
2016 |
No. examined |
586 |
682 |
674 |
699 |
793 |
772 |
668 |
601 |
626 |
724 |
800 |
826 |
8451 |
|
Positive |
205 |
215 |
219 |
221 |
253 |
285 |
229 |
253 |
207 |
227 |
213 |
247 |
2774 |
|
|
P. falcipirum |
180 |
197 |
195 |
191 |
208 |
259 |
197 |
242 |
189 |
215 |
193 |
236 |
2502 |
|
|
P. vivax |
25 |
18 |
24 |
30 |
45 |
26 |
32 |
11 |
18 |
12 |
20 |
11 |
272 |
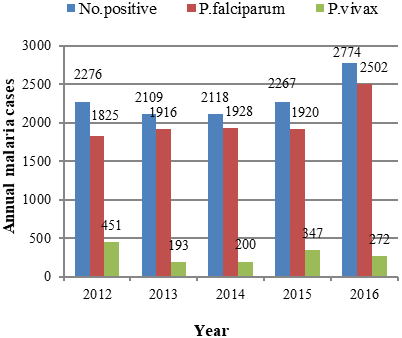
Annual confirmed malaria cases recorded at Dansha town and its surroundings
Over five years, the proportion of species composition in the research locations displayed various trends. Figure 1 shows that relative to Plasmodium vivax, Plasmodium falciparum was more prevalent in the Dansha town and its surrounding kebeles location. Starting from 2012 to 2014, the Plasmodium falciparum was highly increased by 80.2%, 90.8%, and 91.1%, respectively. However, it decreased in 2015 by 84.7% and once again increased rises in 2016 by 90.2%. During 2012, Plasmodium vivax increased by 19.8%, but it decreased starting from 2013 to 2014 by 9.2% and 8.9%, respectively, and once again increased in 2015 by 15.3% and also declined in 2016 by 9.8%. The prevalence rate of malaria decreased in 2013 by 25.7%, increased in 2014 by 28.8%, again decreased in 2015 by 28.4%, and finally increased by 32.8% in 2016.
|
|
|
Figure 1. Annual confirmed malaria cases were recorded in Dansha town and its surroundings from 2012-2016. |
Monthly health recorded data of malaria prevalence from Dansha distinct health center from 2012-2016
Different trends were seen in 2012 about the species makeup of the plasmodium about the monthly average number of cases. The major peak transmission of Plasmodium falciparum mostly occurred in September and November, while the minor transmission of Plasmodium falciparum occurred in March (89 and July. Regarding the monthly distribution of Plasmodium vivax, the major peak transmission occurred in May, but the minor transmission of Plasmodium vivax occurred in September (Table 4).
Different trends were observed in 2013 about the distribution of the plasmodium species relative to the monthly average of the number of cases. The major peak transmission of Plasmodium falciparum occurred in December and November; while minor transmission of Plasmodium falciparum occurred in August and July. Regarding the monthly distribution of Plasmodium vivax, the major peak transmission occurred mostly in February and July, but the minor peak transmission of Plasmodium vivax in May (Table 4).
In 2014, there were varied trends in the plasmodium species composition based on the monthly average of the number of cases. The major peak transmission of Plasmodium falciparum mostly occurred in January and May; while the minor transmission of Plasmodium falciparum occurred in September and August. Regarding the monthly distribution of Plasmodium vivax, the major peak transmission occurred mostly in July, but the minor peak transmission of Plasmodium vivax in February (Table 4).
There were several trends in 2015 about the distribution of the plasmodium species about the monthly average of the number of cases. The major peak transmission of Plasmodium falciparum mostly occurred in June and March; while minor transmission of Plasmodium falciparum occurred in September and December. Concerning the monthly distribution of Plasmodium vivax, the major peak transmission occurred mostly in May, but minor peak transmission of Plasmodium vivax in December (Table 4).
In 2016, there were various trends in terms of the species that make up the plasmodium population about the monthly average of the number of cases. The foremost peak transmission of Plasmodium falciparum mostly occurred in August; while the slight transmission of Plasmodium falciparum occurred in January. Regarding the monthly distribution of Plasmodium vivax, the foremost peak transmission occurred mostly in May, but minor peak transmission of Plasmodium vivax in August and December (Table 4).
Age, sex, and species breakdown of confirmed malaria cases in Dansha town and its surroundings
The prevalence of Plasmodium falciparum was 68.9% in children under the age of five. In contrast, this age group had a 31.1% Plasmodium vivax prevalence. The overall Plasmodium falciparum proportion for the age group of five to nine years was 90.5%, whereas the overall Plasmodium vivax proportion for the same age group was 9.5%. For the age group of ten to fourteen years, the overall Plasmodium falciparum proportion was 85.2%, whereas the overall Plasmodium vivax proportion was 14.8%. Similarly, the overall proportion of Plasmodium falciparum for the age group from fifteen and above years was 87.5 88.4%, while the overall proportion of Plasmodium vivax for the age group from fifteen and above years was 11.6% (Table 5).
Plasmodium falciparum was found in higher concentrations in the years 2013 (90.8%) and 2014 (90.6%), but it was found in lower concentrations in the years 2012 (80.2%) and 2015 (84.7%). A higher proportion of Plasmodium vivax was registered in 2012 (19.8%) and 2015 (15.3%), whereas a lower proportion of Plasmodium vivax was seen in 2013 (9.2%). Males were more affected than females by malaria parasites but differed year to year. The infection rates among males were (66.3%) and females were (33.7%) (Table 5).
Table 5. Distribution of confirmed malaria cases by Age and Plasmodium species type at Dansha town and its surroundings from 2012 – 2016.
|
Age |
Species type |
Years |
|||||
|
2012 |
2013 |
2014 |
2015 |
2016 |
Total |
||
|
<5 |
P. falciparum |
71.6 |
68.9 |
68.4 |
60.2 |
76.7 |
68.9 |
|
P. vivax |
28.4 |
31.1 |
31.6 |
39.8 |
23.3 |
31.1 |
|
|
5-9 |
P. falciparum |
84.9 |
90.6 |
92.9 |
90.6 |
91.7 |
90.5 |
|
P. vivax |
15.1 |
9.4 |
7.1 |
9.4 |
8.3 |
9.5 |
|
|
10-14 |
P. falciparum |
78.6 |
92.4 |
91.7 |
76.9 |
87.6 |
85.2 |
|
P. vivax |
21.4 |
7.6 |
8.3 |
23.1 |
12.4 |
14.8 |
|
|
≥15 |
P. falciparum |
79.9 |
91.5 |
90.6 |
88.9 |
91.4 |
88.4 |
|
P. vivax |
20.1 |
8.5 |
9.4 |
11.1 |
8.6 |
11.6 |
|
Association of prevalence of malaria parasite infections with age and sex at Dansha town and surroundings from 2012 – 2016
The findings demonstrated that the prevalence of malaria parasite infection or species plasmodium was highly correlated with all age groups of malaria cases (P < 0.05), whereas sex was not significantly associated with malaria prevalence (Table 6). Although the prevalence of Plasmodium falciparum was 3.413 times [OR = 3.413, 95% CI: 2.727 – 4.271] more likely higher than the prevalence of Plasmodium vivax among the age group under five years and the prevalence of Plasmodium falciparum were 0.793 times [OR = 0.793, 95% CI: 0.680 – 0.923] less likely to the prevalence of Plasmodium vivax among the age group from five to nine years (Table 6).
The prevalence of Plasmodium falciparum was 1.315 times [OR = 1.315, 95% CI: 1.155 – 1.497] more likely to the prevalence of Plasmodium vivax among the age groups from ten to fourteen years. The prevalence of Plasmodium falciparum was 0.132 times more likely than the prevalence of Plasmodium vivax of malaria species among people from fifteen years (Table 6).
Table 6. Binary logistic regression analysis of malaria prevalence by age and sex in Dansha town and surroundings from 2012 – 2016.
|
Age group |
Species |
Frequency |
Percentage |
Odds Ratio (95% CI) |
P-value |
|
<5 year |
P. falciparum |
287 |
2.5% |
3.413 (2.727 – 4.271) |
0.000 |
|
P. vivax |
129 |
1.2% |
1 |
|
|
|
Subtotal |
416 |
3.7% |
|
|
|
|
5-9 years |
P. falciparum |
2510 |
21.7% |
0.793 (0.680 – 0.923) |
0.003 |
|
P. vivax |
262 |
2.3% |
1 |
|
|
|
Subtotal |
2772 |
23.9% |
|
|
|
|
5-14 years |
P. falciparum |
2685 |
23.3% |
1.315 (1.155 – 1.497) |
0.000 |
|
P. vivax |
465 |
4.1% |
1 |
|
|
|
Subtotal |
3150 |
27.3% |
|
|
|
|
≥15 |
P. falciparum |
4609 |
39.9% |
0.132 |
0.000 |
|
P. vivax |
607 |
5.3% |
1 |
|
|
|
Subtotal |
5216 |
45.2% |
|
|
|
|
Sex |
|
|
|
|
|
|
Male |
P. falciparum |
6816 |
88.9% |
|
0.996 |
|
P. vivax |
850 |
11.1% |
|
1.000 |
|
|
Total |
7666 |
|
|
|
|
|
Female |
P. falciparum |
3275 |
84.2% |
|
0.996 |
|
P. vivax |
613 |
15.8% |
|
- |
|
|
Total |
3888 |
|
|
|
In this study, a total of 11554 confirmed malaria cases were reported from 40742 suspected malaria examined with an overall prevalence of malaria of 28.4% from 2012-2016. This was significantly higher than the survey results of Ethiopia's national malaria prevalence from 2009 (0.3%) to 2013 (0.2%), and a health record-based study conducted in the southern part of Ethiopia reported that 11.45% of 2521 febrile people who visited the health center for treatment tested positive for malaria [25]. It was much higher than the survey results of national malaria prevalence in Ethiopia from 2015 (0.3%) to 2011 (1.3%) in areas below 2,000 m.a.s.l. 11.5% of 384 feverish people who attended the health center in northern Ethiopia, according to research based on health facilities, tested positive for malaria1. This might be due to the seasonal fluctuation of temperature [17], poor housing conditions of household dwellers [26], and inappropriate bed net usage [27]. Other reasons might be altitude variation and climate conditions that may contribute to the breeding site of the malaria parasite. Human behavior, the prevalence of malaria parasites, medical facilities, housing circumstances, jobs, community knowledge, attitudes, and behaviors about malaria transmission, prevention, treatment, and mosquito control are only a few of the variables that affect the spread of malaria [28].
However, an investigation of the incidence of malaria during ten years (2002–2011) undertaken in the northwest of Ethiopia showed that 39.6% confirmed malaria cases were reported out of 59, 208 cases [1].
The current study result was similar to a hospital-based survey conducted in the Arba-Minch town hospital where 34.7% of confirmed malaria cases were reported in all patients who had visited the outpatient department of the hospital and 60% of the total confirmed malaria cases were males [29].
Regarding Plasmodium falciparum, the prevalence rate in this study was 87.4%. This finding is much higher than a study done in Arsi Negelle Health Center, southern Ethiopia [25], Sire Health Center, East Wellaga zone, Western Ethiopia [30], and Kola Diba, North Gondar, and Northwest Ethiopia [1] which were 19.8%, 66.1%, and 75%, respectively. The reason for the fluctuation of the prevalence of P. falciparum in different study areas might be due to seasonal fluctuation of ambient temperature [31], topography and humidity [32], availability of mosquito breeding sites, and absence of an integrated management system [33].
The prevalence of P. vivax in the current study was 12.6%. This is much lower than a study conducted in Arsi Negelle Health Center, southern Ethiopia, Sire Health Center, East Wellaga zone, Western Ethiopia [30] and Kola Diba, North Gondar, and Northwest Ethiopia [1] which were 74%, 30.5%, and 25%, respectively.
In Ethiopia, insecticidal net coverage has increased to 53.3% [34]. Inpatient malaria cases have been reduced by 73% and child deaths by 62% since ITNs have been distributed nationwide, particularly long-lasting insecticide-treated nets (LLITNs) [35]. According to research from rural Côte d'Ivoire [36] and other regions of Africa, high coverage of bed nets, especially those treated with an insecticide (ITNs and LLINs), resulted in a drop in malaria death and morbidity and reduced transmission [37, 38].
The findings of the present study revealed that 85.8% of respondents used ITNs. Several studies indicated that high stability in one place and the use of ITNs significantly reduce the proportion of malaria morbidity and mortality [38]. ITNs possession prevalence in this study was relatively higher than in the study conducted in Iran which is 20% [39]. Without correct use, the mere existence of ITNs in the various houses of the respondents may not be sufficient to protect people against malaria morbidity. This may potentially follow from these observations. Inspections of ITNs have revealed difficulties in using them, including hanging them on the wall without using them and keeping them in packs.
The results of this study also showed that respondents from the study region had a high level of general knowledge of malaria. Nearly the majority of the responders (99.3%) have a sufficient understanding of malaria. Seventy-five. 8% of those surveyed connected malaria to mosquito bites. This may be in contrast to research by 30 in which 63.4% of participants connected malaria to mosquito bites. This outcome was comparable to those of other African nations like Kenya (77.3%) and Kampala (84%) [31].
Knowledge of a community is of paramount importance for the adoption of good practices for health improvement and malaria prevention. Deepen our understanding of the contextual factors that influence people's practice of malaria prevention and treatment to improve the effectiveness of malaria control interventions. For those residing in malaria-risk regions, health education is crucial to enhancing their understanding of the disease, their perceptions of it, and their behavior when seeking out health care [40]. Educated and uneducated people alike know malaria can be prevented. This might mean that malaria knowledge is not fully acquired through formal education. Knowledge of the disease might also come from non-formal sources, such as informal education.
However, the educational status and knowledge of most people living in malarious areas is limited. This might contribute to limited knowledge on how to use impregnated net, malarial treatment, and other preventive measures [41]. As a result, the current research region has a high prevalence of malaria or 28.4%.
Regarding other aspects of knowledge of respondents on malaria, 75.8%, and 92.9% replied that malaria is caused by mosquito bites and biting at night, respectively. This result is consistent with research from Arba-Minch, where 98.2% of respondents said a mosquito bite causes malaria [42], and the Assosa zone, where 95% of respondents said insects bite at night [43]. However, this finding is higher than a study conducted in the Assosa zone by 34, which has shown that less than half (47.5%) of the study participants responded that malaria is caused by mosquito bites. Additionally, 79.9%, 75.4%, and 85.3% of participants in this research thought that malaria could be spread, avoided, and treated, respectively. About 76.5% of them replied that the use of modern medicine is an adequate treatment for malaria. This is almost in agreement with a study by Paulander [44].
Several factors determine malaria transmission, such as human behavior, the presence of malaria parasites, and social and health facility factors. A community's knowledge, attitudes, and practices (KAPs) about malaria causation, transmission, treatment-seeking behavior, and mosquito control activities play a key role in determining malaria transmission rates [40]. Among the factors associated with malaria infections, not using mosquito nets and living around stagnant water seemed to have had an association with the prevalence of malaria in the study area.
Regarding housing conditions, 57.4% of respondents lived in houses that had corrugated iron sheets. The finding showed an association between the presence of malaria with the type of houses. Those who lived in houses having roofs with corrugated iron sheets were 15 times at higher risk, of getting malaria than those who lived under concrete roofs. The cause may be related to building characteristics that are linked to a high prevalence of malaria in the research region, such as an earth roof, tethering cattle within the home, the existence of windows, open eaves, the absence of a separate kitchen, and the presence of a single sleeping chamber. Poorly built homes have a higher risk of contracting malaria, which may be related to their appropriateness for an abundance of indoor vectors. Since homes are where malaria vectors mostly bite and rest, better housing may lower the likelihood of indoor malaria transmission in the research location. However, according to geography, socioeconomics, and specific household circumstances, housing conditions and their influence on the abundance of indoor vectors may differ [26].
CONCLUSION
The study revealed that different households in Dansha town and the surrounding countryside are highly exposed to malaria. In the research region, malaria was present generally at a rate of 28.4% greater than the prevalence of the country (4.1%) and much higher than the survey results of national malaria prevalence in Ethiopia from 2009 (0.3%) to 2013 (0.2%). This might be an indication that different protective measures should be taken in Dansha town and the surrounding countryside by the community as well as the responsible government authorities. Public awareness formation could be important through strong health addition activities incorporated with the community. Identification and elimination of causes of malaria including breeding sites should be strengthened. Reinforced health education should be implemented and it might be a promising as well as tangible measure to further reduce malarial infection. Dynamic participation of the community should be exploited in environmental organizations to control the transmission of malaria.
ACKNOWLEDGMENTS: We acknowledge Dansha Hospital for providing data and the community who participated in the study.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None