Entomology and
Applied Science Letters
Applied Science Letters
 2023
Volume 10
Issue 1
2023
Volume 10
Issue 1

Psychological therapies and medication significantly affect functional improvement, drug adherence, and relapse prevention of bipolar disorder. The present research is a comprehensive investigation of the efficiency of existing psychosocial interventions for treating adult patients with BD in Iran. This systematic review aims to combine the efficiency of evidence-based psychological interventions with improving the clinical and functional outcomes of people with bipolar disorder in Iran. Using PsycINFO, PubMed, ProQuest, Scopus, Google Scholar, and Iranian databases: SID, Noormags, Magiran, Irandoc, Rices, Ensani.ir, a systematic review was carried out since 2000 in respective databases no time and with language restriction to December 2020. Totally 302 papers were identified, and 18 studies met all our inclusion criteria. Five studies of Psychoeducation (PE); four studies of Cognitive behavioral therapy (CBT); four studies of Dialectical behavioral therapy (DBT); three studies of Mindfulness-based cognitive therapy (MBCT), and two studies of Schema therapy (ST). The usefulness of PE and CBT was proven for the relapse prevention of mania episodes, the enhancement of quality of life, and medication adherence, the usefulness of DBT was proven in increasing quality of life and decreasing impulsivity. MBCT reduces impulsiveness and anxiety and increases the quality of Life; ST effectively reduces symptoms and aggression. Using the appropriate and short protocols for Iranian culture to be performed simultaneously on the patients and caregivers of bipolar patients will play an essential role in preventing relapse, drug adherence, and increasing the life quality of bipolar patients.
INTRODUCTION
Bipolar disorder is a chronic disorder including repeated episodes of (hypo) mania and depression, a high relapse rate, and significant comorbidity with other psychiatric disorders [1, 2].
The mood swings of bipolar disorder are so intense that they can cause severe disruptions in social, occupational, and interpersonal functioning. Bipolar disorder is one of the causes of disability among young people [3]. A lack of treatment adherence is a significant factor in treating fractiousness in patients with bipolar disorder. In general, studies show that when the patient does not believe in treatment, there is no long-term adherence to treatment [4].
Because pharmacological treatment can not deal with all the demands of the patients, there is an increasing need to develop and implement affordable and influential interventions tailored to the individual patient [5]. Evidence suggests that psychological intervention can be a helpful tool in improving therapeutic adherence and overall performance in bipolar patients [6]. Successful psychological therapy is a therapy that improves patients' overall performance, increases drug adherence, and prevents recurrence [7]. Various special psychotherapies have been created to bridge the above gaps and better the disease result [8].
According to the evidence, one of the three disabling disorders in Iran is bipolar disorder [9]. The effectiveness of psychological therapies has been studied during extensive research in Iran [10-20]. However, studies have not reached the same results as to which treatment is effective on which outcome. Furthermore, findings produce vast amounts of information scattered due to community samples, measurement tools, and different research projects. Furthermore, it makes it difficult for the researcher to conclude and compare the findings. The main question is which treatment is more effective according to Iranian culture?
The present research is a comprehensive investigation of the efficiency of existing psychosocial interventions for treating adult patients with BD in Iran. This systematic review aims to combine the efficiency of evidence-based psychological interventions with improving the clinical and functional outcomes of people with bipolar disorder in Iran. We do not have a previous systematic review of this to the best of our knowledge. However, a review study has been conducted to investigate the efficiency of patient and family psychological therapies for Severe Mental Disorder (SMD) [9]. Nevertheless, quality assessment studies have not been conducted on it.
A quantitative meta-analysis of the existing evidence was not performed due to the significant discrepancies in interventions and definitions of various outcomes. Alternatively, the present systematic review emphasized a significant investigation of research design, methods, and outcome criteria in the identified Randomized Controlled Trials (RCTs) according to the Cochrane Collaboration's Risk of Bias tool. We targeted studies that examined the effectiveness of psychological interventions to improve functional and clinical results, including relapse prevention, treatment adherence, and Quality of Life (QoL) among patients having bipolar disorder.
MATERIALS AND METHODS
The guidelines of Preferred Reporting Items for Systematic Reviews (PRISMA) were followed [21].
Search strategy
The authors searched PubMed, Scopus, PsycINFO, ProQuest, Google Scholar, and Iranian databases: SID, Noormags, Magiran, Irandoc, Rices, Ensani.ir databases since 2000 in respective databases no time and with language restriction to December 2020. An extra search was performed on Clinicaltrials.gov for registered RCTs to find missing data in the conducted examinations. In addition, a search for published study protocols and IRCT was carried out on related search engines. The primary search criteria were defined based on the mesh term and the PICO framework.
These keywords in Persian and English were utilized to identify psychological interventions included: "Mindfulness-based Cognitive Therapy," “CBT”, "Acceptance and Commitment Therapy", "Problem-solving Therapy", "Behavioral Activation Therapy", "Short-term Psychodynamic Therapy", "Non-directed Supportive Therapy", "IPSRT", "FFT", “Psychotherapy”, "Cognitive-behavioral family intervention", "family therapy", "group therapy", "intensive psychosocial intervention", "functional remediation", "cognitive remediation", and "Interpersonal Therapy." The search terms utilized for bipolar disorder were: “Psychosis AND Manic-Depressive”, “Affective Psychosis AND Bipolar”, “Psychoses AND Bipolar Affective”, "Manic Depressive Psychosis" “Disorder AND Bipolar”, "Manic-Depressive Psychosis" Psychoses AND Manic Depressive”, "mood Disorder" and “Psychoses AND Manic-Depressive”.
The search terms for bipolar disorder and intervention were combined with the Boolean term “AND”. Furthermore, to prevent missing relevant studies, we carried out all the references of the included articles hand searched.
Data on research specifications containing the sample size, city, diagnosis, length, number of sessions, type of intervention, study design, and attrition rate were extracted and presented in two tables.
Inclusion and exclusion criteria
To develop eligibility criteria, the PICOS model was used [22]. Eligible articles were:
Articles that included samples with multiple diagnoses, and were meta-analyses, reviews, meeting abstracts, and case reports were excluded.
Data extraction
Two researchers (M.Y and F. M) independently extracted the data, investigated the quality of eligible studies, and performed double-checks. If necessary, all differences and disagreements were resolved by a third independent investigator (NM. B). A hand-search was conducted by screening and tracking citations in the included articles for eligible articles. In all stages, all papers were regarded by inclusion/exclusion criteria. In all cases, disagreements were reached through discussion with other authors (NM. B).
Quality assessment of studies
The Revised Cochrane risk-of-bias tool (RoB 2) was used to assess the risk of bias [23]. The Cochrane assessment of the risk of bias included: measures of selection bias, performance bias, detection bias, attrition bias, and reporting bias. Two independent researchers (M.Y and F. M) evaluated the quality of the research, and any differences were reconciled by a third researcher (NM.B). Based on the Cochrane Handbook recommendation, researchers were stratified as low risk of bias, high risk of bias, or unclear regarding each domain. In addition, the majority of trials had no deviations from the intended interventions. Also, in 5 trials, the attrition rate was unclear, and two trials had concealment (Table 1).
Statistical analysis
Key findings were summarized in texts, tables, and figures. Though the main plan was to perform a meta-analysis, this was impossible due to the heterogeneity of studies in the type of intervention, duration of follow-up, the number of intervention sessions, the individual's qualifications, and the format of intervention delivery.
Table 1. Risk of Bias for Randomized Controlled Trials, Assessed according to the Revised Cochrane Risk-of-bias Tool for Randomized Trials (RoB 2).
|
Publications |
Randomization process |
Deviations from the intended interventions |
Missing outcome data |
Measurement of the outcome |
Selection of the reported result |
Overall Bias |
|
Ghaderi et al. [24] |
L |
U |
U |
L |
L |
L |
|
Mohammadi et al. [25] |
L |
U |
U |
L |
L |
L |
|
Ghoshchian et al. [26] |
L |
U |
L |
L |
L |
L |
|
Kazemi-Zahrani and Mohagheghian [20] |
L |
U |
L |
L |
L |
L |
|
Afshari et al. [19] |
L |
U |
L |
L |
L |
L |
|
Erfan et al. [27] |
L |
U |
L |
L |
L |
L |
|
Farvareshi et al. [28] |
L |
U |
U |
L |
L |
L |
|
Molavi et al. [29] |
L |
U |
L |
L |
L |
L |
|
Borjali et al. [17] |
L |
U |
L |
L |
L |
L |
|
Rashedi et al. [10] |
L |
U |
L |
L |
L |
L |
|
Talebizade et al. [30] |
H |
U |
U |
L |
L |
H |
|
Bahredar et al. [12] |
L |
U |
L |
L |
L |
L |
|
Masoudi et al. [18] |
L |
U |
L |
L |
L |
L |
|
Hasani et al. [31] |
L |
U |
U |
L |
L |
L |
|
Faridhosseini et al. [11] |
L |
U |
L |
L |
L |
L |
|
Rahmani et al. [32] |
L |
L |
L |
L |
L |
L |
|
Zargar et al. [14] |
L |
U |
L |
L |
L |
L |
|
Javadpour et al. [33] |
L |
L |
L |
L |
L |
L |
L: Low risk of bias; H: High risk of bias; U: unclear
RESULTS AND DISCUSSION
Study selection
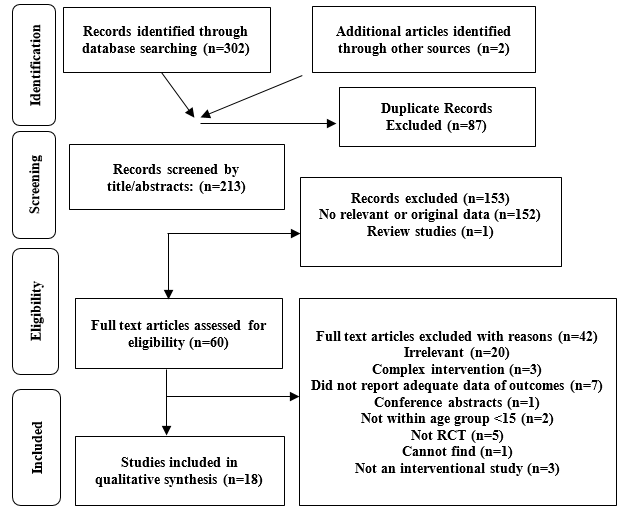
Totally 302 papers were identified from the primary search. Among these, 76 were duplicates and were excluded after screening by title and abstract 153 unrelated studies were discarded because of the initial investigation of inclusion Criteria or unrelated title and review. Moreover, 80 papers were retained for full-text review. Of 80 studies included in the full-text review, of these articles, 62 were excluded due to the following reasons: irrelevant, without a placebo-controlled group, complex intervention, without sufficient data for outcomes, and conference abstracts. Eventually, 18 studies met all our inclusion criteria. The flow chart of the literature search is indicated in Figure 1.
Characteristics of included studies
Selected eligible trials enrolled 761 participants ranging from 18 to 59 years old and were performed in Iran. The participants of 12 studies were females and males except for four pieces of research performed on females and two studies conducted on males. Five studies examined PE [12, 13, 26, 32, 33]; four studies were CBT [19, 25, 29, 30]; four studies were DBT [18, 20, 28, 32] three studies were MBC [19, 30, 31] and two studies were ST [24, 27], but three studies compared the combination of two psychological interventions with Treatment as usual(TAU) [25, 26, 31]. All studies were RCTs. The intervention period was from 4 to 16 weeks—overall follow-up time after the end of the intervention (Table 2).
Candidate psycho-education interventions (PE) (N = 321)
One study randomized control trial investigated the effects of 5 sessions of an individual-based PE (n = 22) and 21 sessions of FFT(n = 22) relative to TAU(n=22) on depression and mania symptoms in BD patient type 1 in Semnan in 2017. The study initially included 75 patients, but only 66 female patients aged 25 -55 years were randomly divided into three groups by lottery method. One experimental group received individual PE, and the other group received FFT. The control group received only medication. All participants completed the study. The results showed that PE alleviated the symptoms of acute depression but did not affect mild symptoms. Moreover, family-focused therapy is most effective in preventing the recurrence of manic symptoms, reducing clinical symptoms, and increasing therapeutic alliance. This study had no attrition [26].
The second study assessed the impact of 10 weekly group sessions PE compared to TAU on drug adherence and the overall performance of bipolar patients type 1 in Shiraz in 2017. 45 BD patients were divided into pharmacology, psychiatric intervention, and placebo groups. Participants 3 to 6 months after the intervention also completed the questionnaires. The results showed that the mean score of drug adherence and overall performance for the PE group was high. PE increases awareness about the disease, and drug effects, and therapy alliance reduces the frequency of recurrences and improves patients' quality of life. The attrition rate was 22.22 [13].
The third study researched the impacts of eight group sessions of PE (n = 13) following Iranian culture compared to TAU (n = 13) on quality of life and the recurrence of bipolar patients in Mashhad in 2014. 26 BD patients aged 18-50 years were randomly divided into two groups. The experimental group received PE twice a week for a month, and the control group received only medication. The measure of the study was assessed at baseline and after 6 months of follow-up. Findings showed that providing information to patients and their family members reduces the recurrence of mania and depression episodes. The attrition rate was 7.69% [12].
The fourth study was a clinical trial to examine the effects of ten group sessions PE compared to TAU on drug adherence of bipolar patients with type 1 in Tabriz in 2016. Seventy-six bipolar patients (women) aged 18-50 years were randomly assigned to experimental and control groups. The experimental group received group sessions PE twice a week. The results indicated a significant within-group improvement in adherence to the PE group's score. According to the results of this study, psycho-education combined with drug therapy is one of the most effective therapeutic components in preventing recurrence and increasing drug adherence in these patients. The attrition rate was 5.55.
The final identified psychological RCT investigated the effects of eight sessions of individual PE (n = 44) compared to TAU (n = 54) on the Quality of Life, relapse rate, and drug adherence in bipolar patients in Shiraz in 2013. 108 BD patients were randomly divided into experimental and control groups. The experimental group received PE for up to 4 weeks, but the control group received only medication. When the study was done, two groups completed the research tools and were followed by telephone follow-up every month for up to 2 years. The present study's findings indicated that patients in the "intervention" group had a statistically significant increase in medication compliance and life quality. As to relapse and hospital admission, the "intervention" group reported much fewer cases than the "control" group at a significance level. The attrition rate was 20.37 [33].
Candidate cognitive behavioral therapy interventions (CBT) (N = 105)
first randomized control trial design investigated the effects of 8 weekly individual CBT (n = 12) in comparison with TAU (n = 12) on reducing the signs and symptoms of BD patients type-I in Ardabil in 2018. Twenty-four bipolar patients were randomly assigned to experimental and control groups. 75% of patients had a history of hospitalization. Patients responded to research tools before and after the intervention. These authors reported that CBT with medication had a significant effect on mania indices. The attrition rate was 4.1 [29].
Quasi-experimental research evaluated the impacts of 16 weekly CBT (n = 8) compared to TAU (n = 7) on preventing the recurrence of bipolar disorder type 1 in Tehran in 2012. 15 BD patients in the partial recovery phase (3 males and 12 females) were randomly assigned to experimental and control groups. Both groups responded to the research tools at the end of the study. Based on the results of this study, the intervention group showed a significant decrease in depression and anxiety symptoms. There was no significant difference between the two groups in mania symptoms and drug adherence. The attrition rate was 7.14 [30].
Another quasi-experimental research evaluated the impacts of 10 weekly sessions of CBT (n = 12) and 12 sessions of ACT (n = 12) compared to TAU (n = 12) on depression, positive and negative symptoms in patients with bipolar disorder in Shiraz in 2020, 36 bipolar patients (12 females and 24 men) were divided randomly into three groups (one control and two experimental groups). Two experimental groups received intervention twice a week. The results showed that both approaches were effective in reducing depression and regulating positive and negative symptoms in BD. However, ACT was more effective than CBT in regulating positive and negative symptoms and reducing depression. The attrition rate was not mentioned [25].
An experimental study investigated the effects of 8-session group CBT (n = 15) in combination with Pharmacotherapy (TAU) (n = 15) on Mania and Depression Symptoms and Awareness of Signs of Relapse in BD Patients in Mashhad in 2009. Thirty women who had bipolar disorder were randomly assigned to two groups and were followed for six months. All subjects were put to a pre-test in similar conditions with measures of scale 2 and 9 of the MMPI Test. The experimental group received CBT twice a week, but the control group received medication. The findings showed that CBT had more effectiveness in reducing mania symptoms and increment awareness of relapse warning signs than the control group. However, there are no significant differences in depression symptoms between the two groups. The attrition rate was 26.66 [19].
Candidate dialectical behavior therapy (DBT) (N = 180)
A quasi-experimental study investigated the effects of 12 sessions of DBT (n = 15) compared to TAU (n = 15) on impulsiveness and quality of Life of Type 1 BD patients in Tabriz in 2018. 30 BD patients (men) in 18-59 were randomly assigned to experimental and control groups. The results showed that DBT improved the quality of Life of BD patients and reduced their impulsiveness by teaching adaptive strategies such as recognizing positive and negative emotions and modulating their thoughts and feelings. The attrition rate was not mentioned [28].
A quasi-experimental study evaluated the impacts of 12 weekly sessions of DBT (n = 20) in comparison with TAU (n = 20) on improving quality of life and reducing Impulsiveness in BD patients (men) in Khorramabad in 2013. 40 BD patients were randomly assigned to control and experimental groups. According to the results, impulsiveness and Self-destruction were reduced significantly, and the experimental group's quality of life was increased. This study had no attrition [18].
Another quasi-experimental study investigated the effects of 12 weekly sessions of DBT (n = 30) compared to TAU (n = 30) on executive function in BD patients in Kashan in 2018. Sixty bipolar patients aged 18-55 were randomly assigned to control and experimental groups. The results showed that DBT reduced the symptoms of depression and improved emotional control and self-efficacy in BD patients. However, the severity of mania symptoms did not decrease in the intervention group. The attrition rate was 16.21 [20].
Another experimental study has examined the effects of 12 weekly sessions of DBT (n = 25) compared to TAU (n = 25) on executive function, emotion control, and Severity of Symptoms in Type 1 BD patients Isfahan 2018. Fifty patients in the age range of 20-45 were divided randomly into experimental and control groups. Both groups completed the research tools before and after the intervention. 64% of the control group and 54% of the experimental group were female. The present study showed that the mania score in the experimental group was reduced significantly, but there was no change in the depression scores of the two groups. The attrition rate was 2% [32].
Candidate mindfulness-based cognitive therapy (MBCT) (N = 95)
A quasi-experimental study evaluated the impacts of 8 sessions of group-based MBCT (n = 20) in comparison with TAU (n = 20) on impulsiveness and self-deterrence of BD patients in Isfahan in 2016. 40 BD patients with a mean age of 39.28 years were randomly assigned to control and experimental groups. The experimental group received intervention twice a week. The results showed that Mbct could be effective in reducing impulsiveness. The attrition rate was 25 [19].
A quasi-experimental was evaluated the impacts of 12 sessions group - based on MBCT (n = 12) combined with 16 sessions of recovery-focused Cognitive Behavioral Therapy (RFCBT) (n = 12) compared to TAU (n = 12) on anxiety and problems in emotion regulation and quality of Life in BD patients in Shiraz in 2018. Participants were divided into three groups. Participants completed research tools before and after the intervention. The results showed that both treatments effectively reduced anxiety symptoms and enhanced the quality of life. MBCT was effective in emotion regulation problems, but there were no significant differences between the two interventions in the degree of effectiveness on these variables. The attrition rate was not mentioned [31].
A quasi-experimental study evaluated the impacts of 8 sessions of group-based MBCT (n = 9) compared to TAU (n = 10) on reducing the severity of depression and manic symptoms of Type 1 BD patients in Tehran in 2013. Patients were assigned to control and experimental groups. The results showed that MBCT is more effective in reducing depression symptoms, but it does not reduce the severity of mania symptoms. The attrition rate was not reported [30].
Candidate schema therapy (N = 60)
A quasi-experimental study investigated the effects of 10 sessions of ST (n = 15) compared to TAU (n = 15) in reducing symptoms and modulating the initial maladaptive schemas of BD patients in Isfahan in 2015. Thirty people (10 men and 20 women) were randomly divided into experimental and control groups. The intervention received ST twice a week. The results showed that this treatment effectively reduced depression and mania symptoms and modified early maladaptive schemas in bipolar patients. This study was not attrition [24].
Emotional schema therapy
A quasi-experimental study investigated the effects of 14 sessions of EST (n = 15) compared to TAU (n = 15) on Impulsiveness and mood symptoms of women with BD in Isfahan in 2016. Thirty patients with bipolar disorder were randomly assigned into two control and experimental groups. The subjects responded to the research tools in 3 stages: pre-test, post-test, and follow-up. The results showed that EST reduced aggression dimensions, and this decrease was stable in the 3-month follow-up. The attrition rate was 6.66 [27].
Table 2. Demographic Characteristics of Included Studies
|
Duration Follow-up (month) |
Attrition rate |
Intervention |
Mode of intervention |
Sessions (n) |
Mean age/Range (year) |
Duration (Week) |
Sample size Experimental /Placebo groups |
Gender |
diagnosis |
Study Design |
Location |
First Author (year) |
code |
|
|
Control group |
Treatment group |
|||||||||||||
|
- |
no |
TAU |
ST |
Individual |
10 |
31.91 |
5 |
15/15 |
Both |
Bmd1, 2 |
Randomized, TAU -controlled, parallel trial |
Esfahan |
Ghaderi (2015) |
1 |
|
- |
unclear |
Waiting list |
CBT, ACT |
Group |
10/12 |
15-25 |
5/6 |
12/12/12 |
Both |
Bmd |
Randomized, TAU -controlled, parallel trial |
Shiraz |
.Mohammadi (2020) |
2 |
|
4 |
no |
TAU |
PE/FFT |
Individual |
5/20 |
25-55 |
5 |
22/22/22 |
Female |
Bmd1 |
Randomized, TAU -controlled, parallel trial |
Semnan |
GhoshchiaS (2017) |
3 |
|
- |
25 |
TAU |
MBCT |
Group |
8 |
39, 28 |
4 |
20/20 |
Both |
Bmd1, 2 |
Randomized, TAU-controlled, parallel trial |
Esfahan |
Kazemi (2016) |
4 |
|
3 |
16.21 |
TAU |
DBT |
Group |
12 |
37 |
12 |
30/30 |
both |
Bmd1, 2 |
Randomized, TAU -controlled, parallel trial |
Kashan |
Afshari (2018) |
5 |
|
3 |
6.66 |
TAU |
ST |
Group |
14 |
32.71 |
14 |
15/15 |
Female |
Bmd1, 2 |
Randomized, TAU -controll, parallel trial |
Esfahan |
Erfan (2020) |
6 |
|
- |
4.16 |
TAU |
DBT |
Individual |
12 |
34 |
12 |
15/15 |
Men |
Bmd1 |
Randomized, TAU -controlled, parallel trial |
Tabriz |
Farvareshi (2018) |
7 |
|
- |
unclear |
TAU |
CBT |
Individual |
8 |
18-50 |
8 |
12/12 |
Both |
Bmd1 |
Randomized, TAU, -controlled, parallel trial |
Ardabil |
Molavi (2018) |
8 |
|
- |
unclear |
TAU |
DBT |
Group |
12 |
20-45 |
12 |
20/20 |
Men |
Bmd1 |
Randomized, TAU-controlled, parallel trial |
Khoram Abad |
Borjali (2013) |
9 |
|
- |
7.14 |
TAU |
CBT |
Group |
14 |
31.5 |
14 |
7/8 |
Both |
Bmd1 |
Randomized, TAU -controlled, parallel trial |
Tehran |
Rashedi (2012) |
10 |
|
- |
unclear |
TAU |
MBCT |
unclear |
8 |
18-65 |
8 |
19 |
Both |
Bmd |
Randomized, TAU-controlled, parallel trial |
Tehran |
Talebizade (2013) |
11 |
|
3-6 |
22.22 |
TAU- PLACEBO |
PE |
Individual |
9 |
18-50 |
9 |
15/15/15 |
Both |
Bmd1 |
Randomized, TAU –placebo-controlled, parallel trial |
Shiraz |
Bahredar (2013) |
12 |
|
6 |
26.66 |
TAU |
CBT |
Groupe |
8 |
26.89 |
4 |
15/15 |
Female |
Bmd |
Randomized, TAU -controlled, parallel trial |
Mashhad |
Masoudi (2009) |
13 |
|
|
Unclear |
Waiting list |
MBCT/RFCBT |
Individual |
12/16 |
36.8 |
6/8 |
12/12/12 |
Both |
Bmd |
Randomized Waiting list -controlled, parallel trial |
Shiraz |
Hassani Ardekani (2018) |
14 |
|
6 |
7.69 |
TAU |
PE |
group |
8 |
28.41 |
4 |
13/13 |
Both |
Bmd |
Randomized TAU -controlled, parallel trial |
Mashhad |
Farid Hosseini (2017) |
15 |
|
- |
5.55 |
TAU |
PE |
Group |
10 |
29.3 |
5 |
38/38 |
Femail |
Bmd |
Randomized(single-blind) TAU -controlled, parallel trial |
Tabriz |
Rahmani (2016) |
16 |
|
- |
2 |
TAU |
DBT |
Group |
12 |
30.96 |
12 |
25/25 |
Both |
Bmd1 |
Randomized TAU -controlled, parallel trial |
Esfahan |
Zargar (2018) |
17 |
|
18 |
20.37 |
TAU |
PE |
Individual |
8 |
18-60 |
8 |
44/54 |
Both |
Bmd |
Randomized TAU-controlled single-blind parallel trial |
Shiraz |
Javadpoor (2013) |
18 |
Abbreviations: PE: Psychoeducation, CBT: Cognitive Behavioral Therapy, DBT: Dialectical Behaviour Therapy, MBCT: Mindfulness-Based Cognitive Therapy, ST: Schema Therapy, ACT: Acceptance and Commitment Therapy.
|
|
|
Figure 1. Flow Chart of the Number of Studies Identified and Selected in the Meta-analysis. |
This study is the first systematic review synthesizing the full range of psychological intervention studies that have been carried out among People suffering from bipolar disorder in Iran.
The present review indicates that the literature supports: the usefulness of PE for the relapse prevention of mania episodes, enhancement of quality of life and medication adherence, and alleviating symptoms of acute depression; unfortunately, it does not affect the mild symptoms of depression [18, 26, 28]. There is controversy about the efficacy of CBT in reducing depression and mania [17, 19]. The usefulness of DBT was proven in increasing quality of life and decreasing impulsiveness. However, there is controversy about its effect on mania and depression symptoms [20, 34]. MBCT reduces impulsiveness, and anxiety, and increases the quality of life but does not affect mania [31]. ST is effective in reducing symptoms and aggression [24, 26, 27].
Studies did not reach the same results: methodological problems, the variety of treatments, and different measuring tools to evaluate the outcomes and competence of intervention performers. Most RCTs suffer from various main methodological challenges, and the bias risk is usually moderate to high, decreasing the quality of research. The majority of RCTs did not distinguish between primary and secondary outcomes. The details of how random allocation and concealment were not described. The sizes of the sample were small in half of the trials [11, 12, 29]. Dropout rates in four trials were n = 5 (> 20%) [11, 17, 19, 35], and only two studies did not have a fall. The research was done in the capital cities of different provinces in Iran (8 provinces out of 31 provinces in Iran), and most of them were performed in Isfahan.
The evidence shows that the severity of the disease has an important role in the outcomes of the disease, and frequent recurrences are associated with weaker outcomes. One of the factors that should be considered in the prognosis and treatment of bipolar disorder is paying attention to the family's role and importance [36]. In most cases in Iran, family members are the primary caregivers, and lack of expression of positive emotion, insufficient information about mental illness due to the stigma, and lack of patient participation in problem-solving due to cultural issues are common [37]. Due to the frequent recurrence and the importance of family attitude to the disease, they need to cope with daily stress [38].
According to the present systematic review results, psycho-education has been the core of the intervention and effectively increases drug adherence and the quality of life. The effects of PE were proven to reduce the recurrence in various internal and external studies [39]. According to the results of previous studies, patients who are in the first stages of the illness and have fewer recurrences benefit more from psychological treatments [40]. Family intervention seems to have significant advantages for patients and caregivers [41]. However, simultaneous intervention seems more effective because caregivers do not have enough information about the disease. Inadequate communication skills, poor problem-solving, and lack of skill in managing daily stress are common [42]. FFT, which was developed by Miklowitcs and had all the above components, was conducted outside of Iran. A few studies In Iran have performed this intervention on patient caregivers [43, 44]. The long sessions of this treatment, the lack of cooperation between families and patients, and the high attrition rate have caused the reluctance of specialists to perform this intervention. Due to the short hospital stay of patients, if the protocol of this treatment is shorter, follows Iranian culture, and can be done by all specialists with any level of education, it will be more practical. It will increase cooperation between patients and families [45].
CONCLUSION
According to the results of previous studies, patients who are in the first stages of the illness and have fewer recurrences benefit more from psychological treatments. Family intervention seems to have significant advantages for patients and caregivers. However, simultaneous intervention seems more effective because caregivers do not have enough information about the disease. Inadequate communication skills, poor problem-solving, and lack of skill in managing daily stress are common. FFT, which was developed by Miklowitcs and had all the above components, was conducted outside of Iran. A few studies in Iran have performed this intervention on patient caregivers. The long sessions of this treatment, the lack of cooperation between families and patients, and the high attrition rate have caused the reluctance of specialists to perform this intervention. Due to the short hospital stay of patients, if the protocol of this treatment is shorter, follows Iranian culture, and can be done by all specialists with any level of education, it will be more practical. It will increase cooperation between patients and families.
ACKNOWLEDGMENTS: We are grateful to the following individuals who communicated with the authors and provided possible information about data from studies, including Dr. Zahra Raisi and Sanaz Ghasemi.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None