Entomology and
Applied Science Letters
Applied Science Letters
 2023
Volume 10
Issue 1
2023
Volume 10
Issue 1

Escherichia coli is a short, polymorphic, gram-negative, rod-shaped bacterium whose non-pathogenic strains are present in the normal intestinal flora. Escherichia is stable in the external environment and can remain viable in soil, water, and feces for up to several months. E. coli produces a variety of enzymes that decompose many carbohydrates and polyhydric alcohols (glucose, galactose, levulose, lactose, maltose, lures, rhamnose, intermittent sucrose, and dulcite, raffinose, salicin, sorbitol, glycerin) with the formation of pyruvates, which then turn into milk, acetic and formic acids. The biochemical properties of E. coli have been studied by many researchers from different countries, but no correlation has been established between their enzymatic activity and pathogenic properties. Colibacillosis is an acute, predominantly intestinal infection caused by certain serovars of the bacterium E. coli. The route of transmission of E. coli is fecal-oral. This article describes in detail the morphological, tinctorial, cultural, and biochemical properties of E. coli, as well as their antigenic structure. In addition, the symptomatology and diagnosis of the course of colibacillosis caused by various groups of E. coli are described.
INTRODUCTION
Colibacillosis is an acute, mainly intestinal infection caused by some serovars of the bacterium Escherichia coli [1]. Colibacillosis manifests itself in the form of enteritis and enterocolitis and can generalize and proceed with extra-intestinal symptoms [2]. The route of transmission of E. coli is fecal-oral. More often, infection occurs when eating infected dairy and meat products. A contact-household route of transmission of intestinal infection is also possible. The diagnosis of colibacillosis is established when E. coli are detected in vomit and feces, and when an infection is generalized - in the blood [3].
Colibacillosis (coli infections) is a group of infections caused by E. coli and occurs with lesions of the gastrointestinal tract, urinary tract, respiratory tract, meninges, and bacteremia. They are more common in young children. Intestinal infections caused by E. coli are the most common: they are the most common cause of diarrhea in infants and adults [4]. Some strains and their toxins cause life-threatening lesions of internal organs [5].
E. coli is a short polymorphic gram-negative rod-shaped bacteria, non-pathogenic strains of which are present in the normal intestinal flora [6]. Colibacillosis is caused by diarrheal serovars (Table 1).
Table 1. Groups of diarrheal serovars
|
Pathogen groups |
Characteristics of colibacillosis |
|
Enteropathogenic |
They cause colibacillosis in children, especially in the first year of life. Infection usually occurs by contact and household means. |
|
Enterotoxigenic |
They cause cholera-like infections, the incidence is high in countries with hot climates and low hygienic cultures. Infection occurs through food and water. |
|
Enteroinvasive |
Enterocolitis is caused by the type of dysentery. Infection occurs by water and food, and the summer-autumn seasonality is noted. They are mainly distributed in developing countries. |
|
Enterohemorrhagic |
Epidemiological data are insufficient for detailed characterization. In the epidemiology of colibacillosis, the main importance is played by hygienic measures, both of a general and individual nature. |
|
Enteroadhesive |
Bacteria do not form cytotoxin, do not penetrate epithelial cells, and do not have plasmid adhesion factor. They got their name due to the rapid attachment to the surface of the cells. |
E. coli are stable in the external environment and can remain viable in soil, water, and feces for up to several months. In food products (especially in milk), they multiply, forming numerous colonies, and easily tolerate drying [7]. E. coli are killed by boiling and the action of disinfectants.
The reservoir and source of infection are sick people or healthy carriers. Persons with colibacillosis caused by enteropathogenic and enteroinvasive E. coli have the greatest epidemic significance in the spread of the pathogen, other groups of bacteria are less dangerous. Patients with colibacillosis caused by infection with enterotoxigenic and enterohemorrhagic E. coli are contagious only in the first days of the disease, while enteroinvasive and enteropathogenic E. coli are isolated by patients for 1-2 (sometimes 3) weeks. Isolation of the pathogen can last quite a long time, especially in children.
The transmission mechanism of E. coli is fecal-oral, most often the food way of infection is realized for enterotoxigenic and enteroinvasive E. coli and household for enteropathogenic E. coli. In addition, an infection can be carried out by water. In children's groups and among people who neglect the rules of hygiene, it is possible to spread E. coli through contact with and household through contaminated hands, objects, and toys. Infection with enterohemorrhagic E. coli often occurs as a result of the consumption of insufficiently cooked meat, and raw unpasteurized milk [8-12].
There is a clinical classification that distinguishes gastroenteric, enterocolitic, gastroenterocolitic, and generalized forms of the disease. The generalized form can be represented by coli-sepsis or damage to various organs and systems by E. coli (meningitis, meningoencephalitis, pyelonephritis, etc.). Colibacillosis can occur in mild, moderate, and severe forms [13, 14].
This article describes in detail the morphological, tinctorial, cultural, and biochemical properties of E. coli, as well as their antigenic structure. In addition, the symptomatology and diagnosis of the course of colibacillosis caused by various groups of E. coli are described.
RESULTS AND DISCUSSION
Morphological, tinctorial, cultural, and biochemical properties of E. coli
According to the morphology, E. coli has the shape of a straight rod, short, relatively thick, with rounded ends, 2–3 µm long, thick 0.6–1.0 µm (Figure 1). They are located singly, less often in pairs, and in the body, they can take a coccus-like form [15]. E. coli stains negatively according to the Gram method, stains well with conventional aniline dyes, and is often bipolar, especially in tissues and exudates [16]. Under the influence of various abiotic factors, they can form L-forms and acquire the ability to pass through bacterial filters.
E. coli is unpretentious in terms of nutrient media, it can grow in the range from 15-55 °C (temperature optimum is about 37-38 °C). It is an aerobe or facultative anaerobe, pH 7.0–7.4. It grows well on ordinary nutrient media - MPA (meat peptone agar), MPB (meat peptone broth); Endo, and Levin media [17]. On MPA, after 24 hours, transparent juicy colonies with a grayish-blue tint are formed, easily merging, with smooth edges and a smooth shiny surface (S-shape) or flat, dry with a slightly wavy edge and a rough surface (R-shape). In BCH, E. coli causes abundant growth with significant and intense turbidity of the medium and the presence of a grayish, easily broken precipitate when shaken, sometimes forming a film on the surface or a parietal ring. When sowing on a medium with gelatin, no liquefaction of the medium occurs. On injection, a grayish-white growth is obtained. Milk coagulates and litmus milk quickly turns pink (formation of acid) and coagulates.
On Levin's diagnostic medium, E. coli forms dark purple or black colonies; on Endo's differential diagnostic medium, lactose-positive strains form raspberry-red colonies with or without a metallic sheen; on McConkey's medium - pink, red (individual strains of E. coli may not ferment lactose and form colorless colonies on the listed media). E. coli colonies of other serogroups are crimson red [18]. Colonies of hemolysin-forming strains are surrounded by a zone of hemolysis on blood agar. The culture is characterized by a fecal odor [19].
E. coli produces a variety of enzymes that decompose many carbohydrates and polyhydric alcohols (glucose, galactose, levulose, lactose, maltose, lures, rhamnose, intermittent sucrose, and dulcite, raffinose, salicin, sorbitol, glycerin) with the formation of pyruvates, which then turn into milk, acetic and formic acids [20]. Pathogenic and non-pathogenic varieties of E. coli do not differ from each other in morphological, cultural, and enzymatic properties, which makes it difficult to identify pathogens of infectious diarrhea [21].
E. coli antigenic structure
The serological classification of E. coli, developed by F. Kaufman, is based on the analysis of O-, K-, and H-antigens. Initially, researchers identified 146 variants of O-antigen, and 88 variants of K-antigen, by the end of the 80s, 171 serological varieties of O-antigen, more than 100 varieties of K-antigen, and 60 varieties of H-antigen were identified in E. coli. Later, 173 O-serogroups and 56 types of E. coli K-antigen, as well as 80 types of H-antigen were identified [22]. However, not all of these varieties of E. coli are capable of causing intestinal infections in animals and humans.
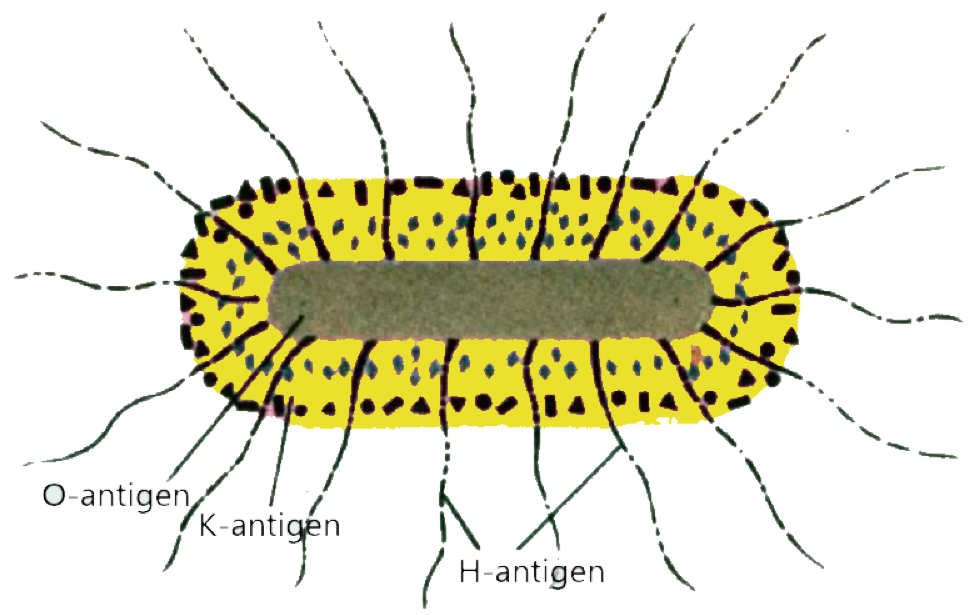
E. coli cells contain three types of antigens: O - somatic; K - sheathed and H - flagellated (Figure 1).
The O-antigen is thermostable (withstands heating at 100 °C for 2.5 hours). It is a lipopolysaccharide-protein complex, heterogeneous, and on its basis, E. coli is divided into groups (more than 160 O-groups) [22].
|
|
|
Figure 1. The structure of E. coli. |
K-antigens surface, shell (acid polysaccharides, rarely proteins). According to their properties, they are divided into three types: L-antigen is thermolabile, inactivated at 100 °C for an hour; In the same conditions, the B-antigen loses its agglutination; A-antigen is thermostable, inactivated at 120 °C for 2.5 hours, is present in the mucous membranes of capsule-forming E. coli O-groups 08,09,020,0101 [23];
The H-antigen is thermolabile, inactivated at 60 °C for 1 hour, the protein is located in the fimbriae (piles) penetrating the cell wall, therefore, recently it is more often called the fimbrial antigen.
K antigens coat O antigen and render E. coli cells innaglutinable in homologous O sera. They have adhesive properties, i.e. with their help, bacteria attach to intestinal epithelial cells.
The H-antigen is flagellated, consists of a thermolabile protein, and has several dozen varieties determined in RA. It is not essential for diagnosis. The combination of O-, K- and H-antigens characterizes the serological variant (serovar) of E. coli [24].
E. coli are resistant to environmental factors. They remain in soil from 6 to 11 months, in water - for up to 300 days, and in manure - for up to 11 months. When stored in semi-liquid agar under a layer of vaseline oil, E. coli retain their pathogenic properties for more than three years. E. coli are unstable to high temperatures. When the medium is heated to 60 °C, they die within 10 min, and at 100 °C, they die instantly. Many disinfectants and substances have a detrimental effect on E. coli: 2.5% formaldehyde solution, 2% solutions of active chlorine and sodium hydroxide, and 3% solution of iodine monochloride [25].
Symptoms and diagnosis of colibacillosis
Enteropathogenic colibacillosis usually develops in young children, the incubation period is several days, manifested mainly by vomiting, loose stools, severe intoxication, and dehydration. There is a possibility of developing a generalized septic form. Adults fall ill with enteropathogenic colibacillosis, and the disease proceeds like salmonellosis [26].
Enteroinvasive colibacillosis is a characteristic course similar to dysentery or shigellosis. The incubation period lasts from one to three days, the onset is acute, there is moderate intoxication (headache, weakness), fever ranging from subfebrile to high values, and chills. Then there are pains in the abdomen (mainly around the navel), and diarrhea (sometimes with streaks of blood, and mucus). Palpation of the abdomen notes pain along the colon. Often, colibacillosis of this type occurs in a mild and erased form, a moderate course can be noted. Usually, the duration of the disease does not exceed a few days [27].
Enterotoxigenic colibacillosis may present with clinical symptoms similar to those of salmonellosis, food poisoning, or resemble a mild form of cholera. The incubation period is 1-2 days, intoxication is mild, the temperature usually does not rise, repeated vomiting is noted, profuse enteric diarrhea, dehydration gradually increases, and oliguria is noted. There are pains in the epigastric region, which are cramping in nature [28].
This infection is often referred to as the "traveler's disease", as it often affects people who have traveled on a business trip or vacation to countries with a tropical climate. Climatic conditions contribute to the occurrence of severe fever with chills, intoxication symptoms, and intense dehydration.
Enterohemorrhagic colibacillosis develops most often in children. At the same time, intoxication is moderate, the body temperature is subfebrile. There is nausea and vomiting, and loose watery stools. In severe cases, by 3-4 days, the disease appears severe pain in the abdomen of a cramping nature, diarrhea intensifies, and in feces that lose their fecal character, an admixture of blood and pus may be noted [29].
Most often, the disease resolves on its own in a week, but in severe cases (especially in young children) on days 7-10, after the disappearance of diarrhea, there is a possibility of developing hemolytic-uremic syndrome (a combination of hemolytic anemia, thrombocytopenia, and acute renal failure). There are frequent violations of brain regulation: cramps of the limbs, muscle rigidity, impaired consciousness up to stupor, and coma. The lethality of patients with the development of these symptoms reaches 5% [30].
Complications
Colibacillosis is usually not prone to complications. In the case of an infection provoked by the pathogen of the Enterohemorrhagic group of E. coli, there is a possibility of complications from the urinary system, hemolytic anemia, and cerebral disorders [31].
Diagnostics
For the diagnosis of colibacillosis, the pathogen is isolated from feces and vomit, in cases of generalization - from blood, urine, bile, or cerebrospinal fluid. After that, a bacteriological examination is performed, sowing on nutrient media. Due to the antigenic similarity of the causative agents of colibacillosis with the bacteria that make up intestinal normocinosis, serological diagnosis is not very informative.
In some cases, the detection of bacterial toxins in the feces of patients can be used. With this type of colibacillosis, signs of hemolytic anemia, and an increase in the concentration of urea and creatinine can be noted in the blood test. Urinalysis usually shows proteinuria, leukocyturia, and hematuria [32].
Prevention
Colibacillosis - a disease associated with low hygienic culture. Personal prevention of these infections is to follow hygiene standards, especially when communicating with children, and washing hands, food, toys, and household items. General prevention is aimed at monitoring compliance with the sanitary and hygienic regime in children's institutions, food industry enterprises, and medical institutions, as well as control over the flow of sewage waste and the state of water sources [33].
Patients after the transfer of colibacillosis are discharged from the hospital after clinical recovery, as well as the results of a threefold bacteriological test. Admission to the team of children who have been in contact with the patient is also carried out after bacteriological diagnosis and confirmation of the absence of isolation of the pathogen. Persons excreting pathogenic E. coli are subject to isolation for the entire period of contagiousness. Food industry workers are subjected to regular examinations for the isolation of the pathogen, in case of a positive test, they are suspended from work [34-38].
CONCLUSION
Different groups of E. coli cause the course of colibacillosis with different symptoms and varying degrees of severity. Enteropathogenic colibacillosis usually develops in young children, the incubation period is several days, manifested mainly by vomiting, loose stools, severe intoxication, and dehydration. Enteroinvasive colibacillosis proceeds like dysentery or shigellosis. The incubation period lasts from one to three days, the onset is acute, there is moderate intoxication (headache, weakness), fever ranging from subfebrile to high values, and chills. Then there are pains in the abdomen (mainly around the navel), and diarrhea (sometimes with streaks of blood, and mucus).
Enterotoxigenic colibacillosis is manifested by clinical symptoms similar to those of salmonellosis, food poisoning, or a mild form of cholera. The incubation period is 1-2 days, intoxication is mild, the temperature usually does not rise, repeated vomiting is noted, profuse enteric diarrhea, dehydration gradually increases, and oliguria is noted. Enterohemorrhagic colibacillosis develops most often in children. At the same time, intoxication is moderate, the body temperature is subfebrile. There is nausea and vomiting, and loose watery stools. In severe cases, by 3-4 days, the disease appears severe pain in the abdomen of a cramping nature, diarrhea intensifies, and in stools that lose their fecal character, an admixture of blood and pus may be noted.
ACKNOWLEDGMENTS: The authors are thankful to colleagues from Stavropol State Medical University who kindly supported the work.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None